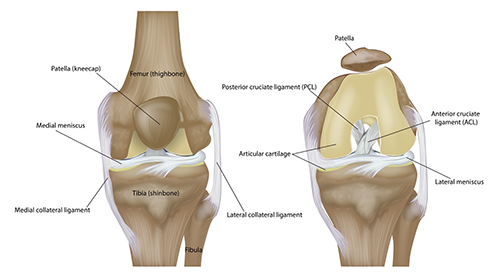
What is the ACL?
The anterior cruciate ligament (ACL) of the knee is one of the ligaments attaching the femur to the tibia. It is in the central aspect of the knee. Its main function is to prevent forward motion (anterior translation) of the tibia in relation to the femur. It also aids in preventing hyperextension as well as internal and external rotation of the knee.
How is the ACL injured?
The ACL is primarily injured during landing, cutting and pivoting type activities. This explains its high association with sporting events such as basketball, soccer, football, and skiing. Injuries to the ACL can happen with or without external contact to the knee at the time of injury.
What are the symptoms of an ACL tear?
Tearing of the ACL can lead to pain, swelling, stiffness, and feelings of instability in the knee. The pain itself may not be localized to a single area of the knee. However, the ACL itself has very few pain fibers so some people may experience minimal pain and swelling if there are no other associated injuries.
How is an ACL tear diagnosed?
Diagnosis begins with a history and physical examination. Physical examination maneuvers such as the anterior drawer test, the Lachman test, and pivot shift test are used to test for ACL laxity. X-rays are used to evaluate the presence of a fracture associated with ACL tears (Segond fractures) or the presence of associated injuries. Finally, an MRI (magnetic resonance image) is used to give the highest quality image of the soft tissues of the knee, including the ACL.

Figure 1. Knee x-ray showing Segond Fracture consistent with ACL tear
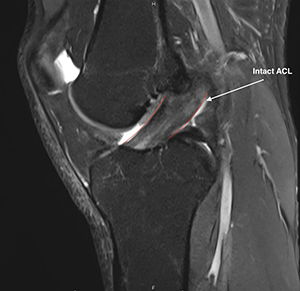
Figure 2. Example of knee MRI with intact ACL

Figure 3. MRI example of knee with ACL tear
What are the treatment options for an ACL tear?
Treatment options are always individually tailored. Considerations include age, activity level, type of activity, how recent the injury occurred, partial versus complete tear, prior treatment, and associated injuries.
Historically, ACL reconstruction has been the gold standard for complete ACL tears. Due to the ACL's location within the knee it has been seen to have limited ability to heal. However, there is some data showing that in select patient populations conservative care with rehabilitation and bracing may be sufficient. There is data to suggest that conservative care does lead to inferior outcomes for children and adolescents. It should also be noted that in nearly all studies comparing outcomes between conservative and surgical care, the surgically treated knees showed increased stability. There are also small case series showing healing of ACL tears with the addition of biologics such as platelet rich plasma.
Surgical options for ACL tears include both ACL repair and ACL reconstruction. ACL repair attempts to heal the ACL tissue whereas ACL reconstruction removes the torn ACL and replaces this tissue with a graft. Determination of candidacy for repair versus reconstruction will depend on the age of the patient, location of the tear, quality of the remaining ACL tissue, and length of time from the injury.
Surgical repair is seen as an alternative to reconstruction due to the goals of limiting ACL graft harvest site morbidity and retaining the patient's native ligament. Typically repairs are ideal for young, active patients with proximal ACL ruptures or single bundle partial ACL ruptures. New advances such as the development Bridge-Enhanced Anterior Cruciate Ligament Restoration graft have attempted to expand these indications. Current outcomes of repair versus reconstruction show similar patient reported outcomes in the short and mid term but with a slightly higher retear rate in the repair group.
ACL reconstruction involves removal of the torn ACL with placement of an autograft (the patient's own tissue) or allograft (use of donor tissue). This treatment option results in improved stability to the knee after surgery, low re-tear rate, and high return to activity. However, rehabilitation and recovery are often extended, lasting six months to a year or longer in some cases.
Treatment options are similar for partial ACL tears. Consideration is given to patient age, percent of ACL tearing, location of ACL tearing, time from injury, laxity of the ACL on examination and activity level. Again, young more active patients trend to worse outcomes with conservative care of partial ACL tears. Surgical repair may serve a larger role in this cohort in comparison to reconstruction.
How is ACL repair performed?
The surgery is performed under a general anesthetic typically with the use of a regional nerve block. ACL repair is performed using an arthroscopically assisted method. It involves placing sutures within the remaining ACL tissue and then anchoring the tissue along with the Bridge Enhanced ACL Restoration collagen graft to both the femur and tibia. Attachment to the femur and tibia can be accomplished with either anchors or suture buttons with drill tunnels.
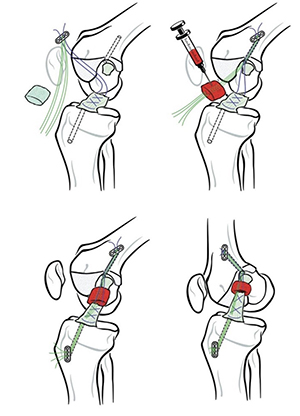
Figure 4. Example of ACL repair technique using the Bridge Enhance ACL Restoration graft (Shah et al. 2025)
How is ACL reconstruction performed?
The surgery is performed under a general anesthetic typically with the use of a regional nerve block. An ACL graft is prepared using either the patient's own tissue or donor tissue. Potential graft harvest sites include the quadriceps tendon, bone-patella tendon-bone graft, and hamstring. Currently, the majority of my patients undergo a quadriceps autograft ACL reconstruction. A drill tunnel is made in both the femur and tibia and the graft is then secured in the bone tunnels to allow for healing.
Figure 5. Step 1- Harvest and prepare quadriceps autograft. (Picture Credit: Arthrex.com)
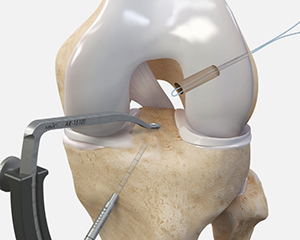
Figure 6. Step 2- Drill femoral and tibial tunnels. (Picture Credit: Arthrex.com)
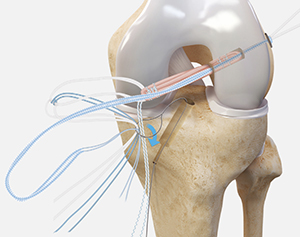
Figure 7. Step 3- Pass and seat the graft in bone tunnels. (Picture Credit: Arthrex.com)
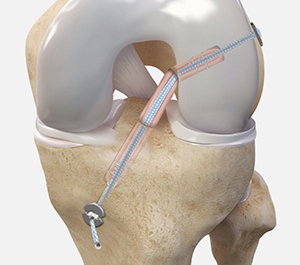
Figure 8. Final graft fixation. (Picture Credit: Arthrex.com)
Graft options for ACL reconstruction
Two main groups of graft for ACL reconstruction include autograft (the patient's own tissue) and allograft (donor tissue). Advantages autograft include improved biologic fixation, lower retear rate, lower risk of rejection. Disadvantages include morbidity from the donor site, harvest site weakness, and harvest site recovery time. Use of allograft has the advantage of no donor site morbidity, shorter surgical time, and possibly reduced post operative pain. Disadvantages include slower biologic incorporation, high re-rupture rates, potential for immune response.
Common autograft harvest sites include the quadriceps tendon, bone-patella tendon-bone, and hamstring. The large majority of my current patients undergo quadriceps autograft reconstruction. Advantages include a larger graft size, potentially biomechanically stronger, and low graft site harvest pain. Disadvantages include possible donor site morbidity, recovery and graft defect.
Other possible procedures at the time of surgery:
Lateral Extra articular tenodesis- This procedure involves taking a portion of your iliotibial band and routing around the lateral collateral ligament of the knee and attaching to the femur. This adds additional constraint to the knee. This procedure may be added in cases depending on the patient's age, activity level, type of activity, and if this is a revision ACL reconstruction.

Figure 9. Example of Lateral Extra Articular Tenodesis. (Picture Credit: Arthrex.com)
Timing of ACL surgery
Many patients want to have surgery as soon as possible to hasten the recovery process. However, there is data to support attending physical therapy prior to surgery. This may be termed "prehab" and can lead to improved strength, functional outcomes, and return to sport after ACL surgery is completed. Some studies also suggest an extended delay to reconstruction may result in an increase in other soft tissue injuries. In some cases, certain associated injuries may preclude delaying surgery. Again, timing is on a case-by-case basis.
Outcomes of ACL surgery
Overall outcomes following ACL reconstruction are generally good to excellent. The following table, although from one study, shows a representation of expected outcomes. The scale is from 0 - 100 with 100 being a perfect score with no knee issues.
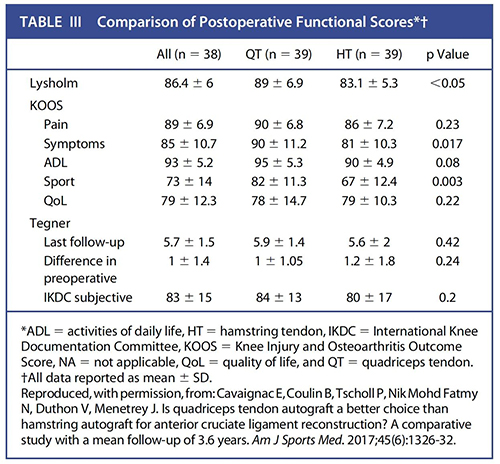
Figure 10. Table III from Marcaccio et al. JBJS REVIEWS 2023;11(10):e23.00057
Return to sport after ACL surgery
Readiness to return to sport after ACL surgery is multifactorial and depends largely on physical, psychological and neurological readiness. Although the outcomes of ACL surgery are generally good to excellent to return to sport rate varies depending on the series reported from ~70-90%. The rate of patients returning to the same level of activity is lower at ~50-60%. Although some patients have returned to sport as soon as 6 months after surgery, there is data to suggest that a return to sport after 9 months can reduce the reinjury rate.
What are possible complications of ACL surgery?
Infection
An uncommon complication reported rates range from 0.1% to 2.4%. Prevention at the time of surgery includes the surgical sterilization of the skin and using the use of antibiotics at the time of surgery. Presentation of infections could include fever, chills, increased pain and swelling at the surgical site, redness, warmth and drainage. Management often includes antibiotics and possibly surgical irrigation and debridement.
Graft Failure
Incidence of graft failure ranges from 2-10% depending on the series reported and graft selection. Prevention includes appropriate surgical technique, rehabilitation, recovery and timing to return to activity. Treatment of graft failure includes revision ACL reconstruction.
Knee Stiffness
Knee stiffness results from scar tissue formation leading to restricted range of motion and can occur in up to 5-10% of cases. Prevention includes timing to surgery and accelerated rehabilitation protocols. Treatment of knee stiffness includes rehabilitation, surgical lysis of adhesions and manipulation under anesthesia.
Deep Venous Thrombosis (Blood clot)
Although typically rare with reports being lower than 1% of cases, there are studies reporting asymptomatic blood clots in up to 15% of ACL cases. Presentation of a blood clot can include increased pain and swelling in the leg with diagnosis confirmed with an ultrasound. Prevention includes early immobilization, possible use of compression stockings, and possible use of chemical prophylaxis such as aspirin. Treatment typically includes use of anticoagulation medications such as lovenox or apixaban.
Nerve injury
Nerve injury is uncommon after ACL surgery. Most common type of nerve injury includes numbness around incision sites. This usually resolves with continued observation. In rare case pain management may be required to aid in symptom management.
Hardware Irritation
Hardware is used to secure the ACL graft to the femur and tibia. Uncommonly this hardware can cause continued pain in the area it is located. This can present as localized pain and swelling at the hardware sites. In such cases the hardware may need to be surgically removed once the graft has fully healed.
Anterior Knee Pain
Persistent anterior knee pain has been historically been associated with bone patella bone graft harvest with rates up to ~40%. Although still possible with hamstring or quadriceps autograft harvest the rates seen are typically much lower with series usually showing rates > 10%. Treatment can include physical therapy, bracing, taping, or possible injections.
Osteoarthritis
Osteoarthtis development after an ACL injury is multifactorial and ultimately related to cartilage injury. Some studies report up to 50% of patients may develop arthritis of the injured knee within 15 years of the injury, although not all of these cases are symptomatic. Prevention includes rehabilitation focusing on quadriceps strengthening and resorting joint mechanics and stability. Treatment may include anti inflammatory medications, injection therapy, rehabilitation and possible joint preservation surgery.
This is not an exhaustive list of all complications. Other complications, although uncommon, can still occur.
What will help my pain after surgery?
Medications including narcotic pain medications and anti inflammatories may be prescribed after surgery to help reduce pain. Nerve blocks at the time of surgery have been shown to be affective at reducing pain with low risk of long term deficits. Additionally, use of cold compression devices have been shown to reduce pain and need for pain medications.
Are there other modalities that can improve my healing after ACL surgery?
There are studies that show use of biologics such as platelet rich plasma can decrease of knee arthrofibrosis and increase speed for graft incorporation into bone after surgery. This can be injected at the time of surgery or after.
Neuromuscular Electrical Stimulation is used during knee rehabilitation to aid in muscle fiber recruitment. This can be applied both at home and during physical therapy sessions.
Use of blood flow restriction therapy involves use of a tourniquet like cuff placed on the lower extremity during exercise. Use of blood flow restriction therapy with low intensity exercise allows lower knee joint pain in comparison to high intensity training without blood flow restriction. This will be used during physical therapy sessions. Check with your physical therapy location if they have this modality available.
Supplement recommendations are often sought after surgery. There is low evidence to support the use of protein supplementation after ACL surgery. No evidence is available to provide recommendations for a particular protein supplement. No significant evidence is available to support creatine supplementation or vitamin supplementation.
Hyperbaric oxygen therapy has long been studied in regard to wound healing. Studies show improved wound healing with the use of hyperbaric oxygen therapy. There is limited data specifically in regard to ACL or knee injuries with hyperbaric oxygen therapy, although there is some animal data to support the use for increased graft incorporation, maturation and healing. There are no specific number of treatments or specific protocols that can be recommended at this time. Hyperbaric oxygen therapy centers are available in Austin.
Do I need to use a brace after ACL surgery?
In the immediate post operative period you will use a knee brace. The use of a knee brace that can lock in extension can prevent knee buckling while walking in the immediate post operative period . It can also be used to prevent excessive knee flexion if other procedures, such as meniscus repair, require limited knee range of motion.
The use of knee bracing when return to sport is controversial. Functional knee bracing has been shown to have benefits in proprioception and limb symmetry. However, clinical studies show no significant benefit in functional stability, patient reported outcomes or retear rates. In contrast there is data to support lower retear rates in skiers post ACL surgery. Your use of a brace will largely be determined on subjective stability, sporting type and activity level.
When can I return to work after surgery?
Return to work will largely depend on your specific occupational requirements. Many patients are no longer requiring the use of pain medications during the day by the fifth day after surgery. If your work is sedentary, you may be able to return as soon as this time. If you are required to stand for a significant period during the day return to work may need to be delayed until you are off crutches. This may be from week 1-6 after surgery depending on other concomitant procedures such as meniscus repair performed. Work that involves heavy lifting may require longer periods away from work if light duty is not available.
When can I drive after surgery?
There is no definitive test we can do to determine when a patient is safe to return to driving. You should not be taking narcotic or sedating medications prior to driving. Studies attempting to look at when it is safe to return to driving have looked at brake response times. In general, brake response time has been shown to return to normal by 4-6 weeks after right sided ACL surgery and 2-3 weeks after left sided ACL surgery. Procedures that result in delayed weight bearing, such as meniscus repair, will likely delay return to driving.
Post operative Instructions
- Following your stay in the recovery room and when your vital signs are stable you will be discharged to your escort.
- Remember, it is normal to feel a little dizzy or drowsy for several hours after surgery. This is due to the action the medicine used during surgery.
- If you do not have a post operative appointment scheduled, please call the office as soon as possible to schedule this appointment.
- Take your pain medicine as directed. Begin the pain medicine before you start getting uncomfortable, as the nerve block will wear off. If you wait to take your pain medication until the pain is severe, you will have more difficulty in controlling the pain.
- Take 1 tablet (81 mg) of aspirin per day, starting the day after surgery and continuing for 4 weeks. The risk of blood clots is quite low after ACL surgery but aspirin is taken as a precaution to decrease the risk. Certain factors such as smoking, birth control pills and certain medical conditions increase the risk of blood clots and it is especially important to take the aspirin for those situations. If you were previously on a blood thinner you will resume this medication, rather than starting aspirin, beginning the day after surgery.
- If you are taking narcotic pain medication you may need a stool softener to prevent constipation. Over-the-counter medication such as Docusate or Milk of Magnesia is recommended.
- Notify the office of any fever, chills, or temperature > 100.5.
- Notify the office of any wound drainage.
- You can begin the home exercises listed below the day after surgery. Perform the ankle pumps periodically, throughout the day. The remainder of the exercises can be performed once at least once a day.
Post-Surgery Diet
Resume your diet as tolerated and include vegetables, fruits, and proteins (such as meats, fish, chicken, nuts, and eggs) to promote healing. Also, remember to have adequate fluid intake. It is common after surgery to lack an appetite. This may be the result of anesthesia and the medications. Proper nutrition is needed for healing. During the healing process, the body needs increased amounts of calories and protein. Eat a variety of foods to get all the calories, proteins, vitamins, and minerals you need. If you have been told to follow a specific diet, please follow it.
If you're not eating well after surgery, contact your healthcare provider about nutritional supplements.
How should I manage my surgical site and bandages?
You can remove your surgical dressing on the third day after your surgery. You will remove everything except the Steri-strips if present. See picture below for example of Steri strips.
Allow the steri-strips to fall off on their own. If necessary, sutures will be removed at your first post-operative visit.
Example of Steri strips:

You may shower with a waterproof bandage covering the incisions in three days. Example of waterproof bandage shown in picture below. These can typically be purchased at CVS or Walgreens. Keep the incisions dry until the Steri strips fall off or are removed in clinic. Try not to let the direct spray of water from the showerhead hit the incision.
You can cover your incision with a bandage if needed to prevent irritation with clothing.
A small amount of drainage from the surgical sites is common. If this occurs, you may apply a bandage to the affected area.
Leakage immediately after surgery is normal and helps to drain some of the fluid that accumulates in the joint during surgery.
The dressings may become moist or blood-stained; this is normal and not typically a cause for alarm.
Example of waterproof bandage:

Do I need to wear a knee brace?
You will use a knee brace such as this:

Instructions for fitting and adjustment can be found at:
https://www.breg.com/products/knee-bracing/post-op/t-scope-premier-post-op-knee-brace/
You will lock the brace straight when walking but can unlock the brace at rest. The prescribed range of motion settings will be set in the operating room.
You may remove the knee brace for exercises as prescribed by the surgeon/therapist, icing, dressing, and showering.
What is my activity level after surgery?
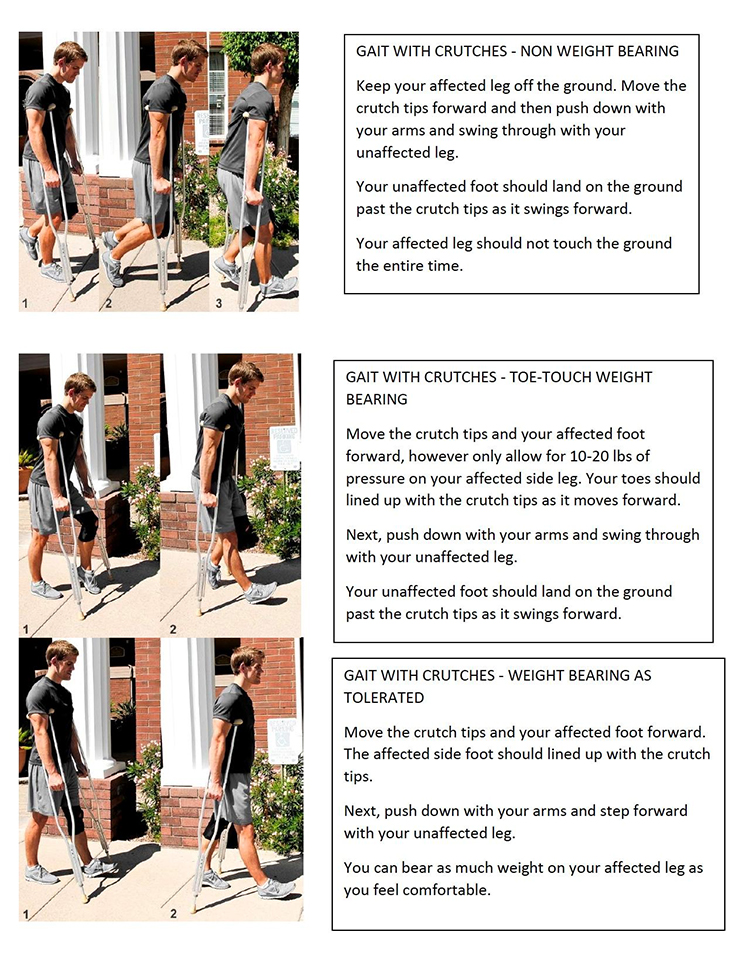
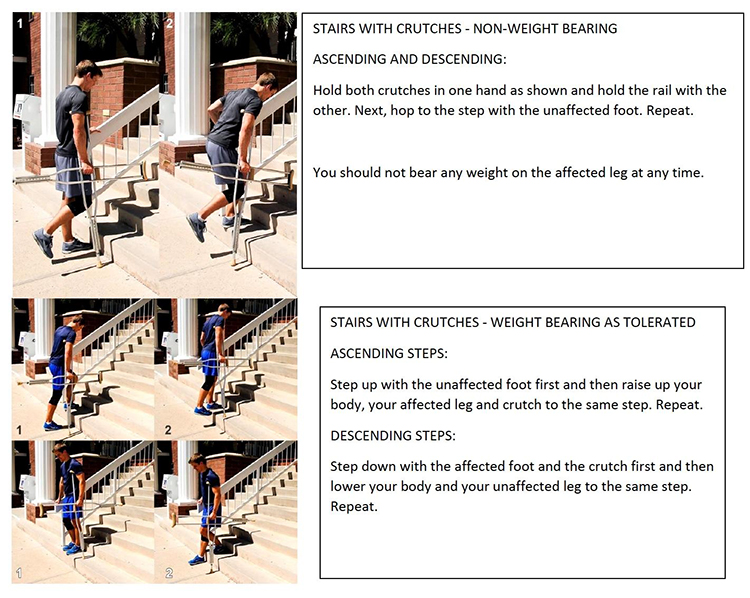
You will use crutches to aid with walking after surgery.
Elevate the operative leg to chest level whenever possible to decrease swelling. Do not place pillows under knees (i.e. do not maintain knee in a flexed or bent position) but rather place pillows under foot/ankle.
Do not engage in activities which increase knee pain/swelling (prolonged periods of standing or walking) over the first 7-10 days following surgery.
Avoid long periods of sitting (without leg elevated) or long distance traveling for 2 weeks.
Physical therapy should begin by post-operative day 5 or sooner.
You can begin motion of your ankle and toes now.
How do I use my ice machine?
Use of cold compression can help with post operative pain and swelling after surgery. One example is the following:

Instructions for use can be found at:
https://www.breg.com/products/cold-therapy/devices/polar-care-wave/
If you have another machine please check that manufacturer's website for use instructions.
Use every waking hour for 15 minutes for the first 24 hours. After this time you can use the machine at least three times a day for 15 minutes.
Do not sleep with the automated device on.
Keep a layer of fabric between the skin and icing device at all times.
How do I use the neuromuscular electrical stimulation?
An example of an NMES machine includes:
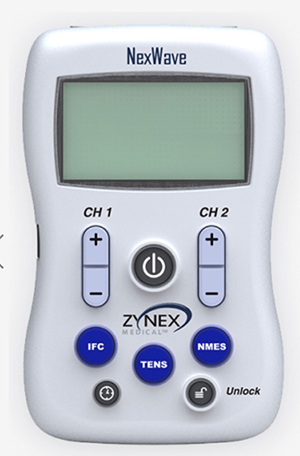
Instructions for use can be found at:
https://www.zynex.com/products/nexwave/
Electrodes will be placed at the quadriceps. For example:
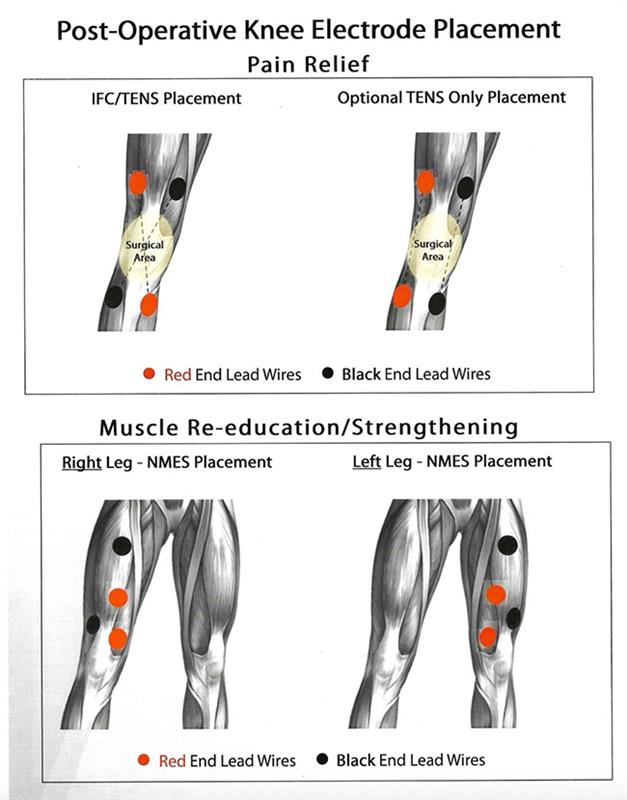
With the knee in extension, increase the stimulation amplitude until contraction of the quadriceps is visualized. Increase amplitude to your tolerance level. Contractions should last 10 seconds with 30-50 second rest periods between contractions. This can be started once the bandages are removed on the third day after surgery. This can be performed at least 5 days a week for one hour per day.
Can I smoke following surgery?
You should not smoke after surgery as it interferes with healing.
Questions or Concerns
If at anytime you have questions or concerns you can either contact your surgeon's medical assistant via email or you can call the main office numbers at: 855-624-3306. You can also use the electronic medical record's online portal to send questions.
Exercises you can perform at home at this time:

Straight Leg Raise
While lying on your back, raise up your leg with a straight knee. Keep the opposite knee bent with the foot planted on the ground.
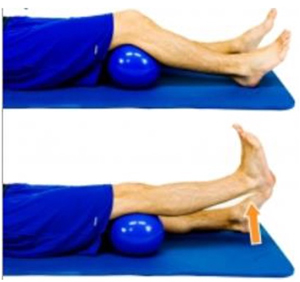
Short Arc Quad
Place a rolled up towel or object under your knee and slowly straighten your knee as you raise up your foot.
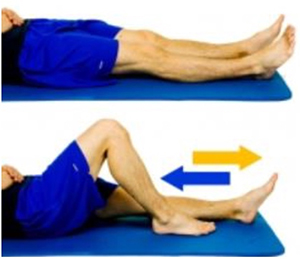
Heel Slides- Supine
Lying on your back with knees straight, slide the affected heel towards your buttocks as you bend your knee. Hold a gentle stretch in this position and then return to original position.
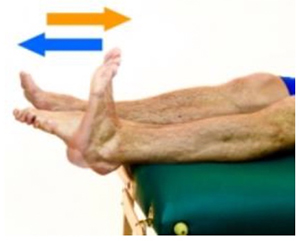
Ankle Pumps
Bend your foot up and down at your ankle joint as shown.
References:
- Greif DN, Emerson CP, Allegra P, et al. Supplement Use in Patients Undergoing Anterior Cruciate Ligament Reconstruction: A Systematic Review. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2020;36(9):2537-2549. doi:10.1016/j.arthro.2020.04.047
- Zakharia A, Zhang K, Al‐Katanani F, et al. Prehabilitation prior to anterior cruciate ligament reconstruction is a safe and effective intervention for short‐ to long‐term benefits: A systematic review. Knee Surgery, Sports Traumatology, Arthroscopy. Published online April 25, 2025. doi:10.1002/ksa.12631
- Simonsson R, Piussi R, Högberg J, Sundberg A, Hamrin Senorski E. Rehabilitation and Return to Sport After Anterior Cruciate Ligament Reconstruction. Clin Sports Med. 2024;43(3):513-533. doi:10.1016/j.csm.2023.07.004
- Leite CBG, Tavares LP, Leite MS, Demange MK. Revisiting the role of hyperbaric oxygen therapy in knee injuries: Potential benefits and mechanisms. J Cell Physiol. 2023;238(3):498-512. doi:10.1002/jcp.30947
- Jones MW, Cooper JS. Hyperbaric Therapy for Wound Healing.; 2025.
- Filbay SR, Dowsett M, Chaker Jomaa M, et al. Healing of acute anterior cruciate ligament rupture on MRI and outcomes following non-surgical management with the Cross Bracing Protocol. Br J Sports Med. 2023;57(23):1490-1497. doi:10.1136/bjsports-2023-106931
- Brinlee AW, Dickenson SB, Hunter-Giordano A, Snyder-Mackler L. ACL Reconstruction Rehabilitation: Clinical Data, Biologic Healing, and Criterion-Based Milestones to Inform a Return-to-Sport Guideline. Sports Health: A Multidisciplinary Approach. 2022;14(5):770-779. doi:10.1177/19417381211056873
- Welling W. Return to sports after an ACL reconstruction in 2024 - A glass half full? A narrative review. Physical Therapy in Sport. 2024;67:141-148. doi:10.1016/j.ptsp.2024.05.001
- Turk R, Shah S, Chilton M, et al. Return to Sport After Anterior Cruciate Ligament Reconstruction Requires Evaluation of gt;2 Functional Tests, Psychological Readiness, Quadriceps/Hamstring Strength, and Time After Surgery of 8 Months. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2023;39(3):790-801.e6. doi:10.1016/j.arthro.2022.08.038
- Petit CB, Slone HS, Diekfuss JA, et al. Sex-Specific Outcomes After Anterior Cruciate Ligament Reconstruction Using an All-Soft Tissue Quadriceps Tendon Autograft in a Young Active Population. Am J Sports Med. 2024;52(10):2450-2455. doi:10.1177/03635465241262018
- Belk JW, Littlefield CP, Smith JRH, et al. Autograft Demonstrates Superior Outcomes for Revision Anterior Cruciate Ligament Reconstruction When Compared With Allograft: A Systematic Review. Am J Sports Med. 2024;52(3):859-867. doi:10.1177/03635465231152232
- Prentice HA, Chan PH, Paxton EW, Felson DT, Funahashi TT, Maletis GB. Patient and Operative Risk Factors for Osteoarthritis After Primary Anterior Cruciate Ligament Reconstruction: A Cohort Study of 41,976 Patients. Am J Sports Med. 2024;52(10):2482-2492. doi:10.1177/03635465241261357
- Heffner M, Chang RN, Royse KE, Ding DY, Maletis GB. Association Between Graft Type and Risk of Repeat Revision Anterior Cruciate Ligament Reconstruction: A Cohort Study of 1747 Patients. Am J Sports Med. 2023;51(6):1434-1440. doi:10.1177/03635465231166084
- Zhou H, Liu H, Lin M, et al. Hyperbaric oxygen promotes bone regeneration by activating the mechanosensitive Piezo1 pathway in osteogenic progenitors. J Orthop Translat. 2024;48:11-24. doi:10.1016/j.jot.2024.07.001
- Allende F, Allahabadi S, Sachdev D, et al. Comparing Clinical Outcomes and Knee Stability in Remnant- Preserving ACL Reconstruction Versus Standard ACL Reconstruction: A Systematic Review and Meta-analysis. American Journal of Sports Medicine. Published online December 1, 2024. doi:10.1177/03635465231225984
- Leite CBG, Leite MS, Varone BB, et al. Hyperbaric oxygen therapy enhances graft healing and mechanical properties after anterior cruciate ligament reconstruction: An experimental study in rabbits. Journal of Orthopaedic Research. 2024;42(6):1210-1222. doi:10.1002/jor.25787
- Banovetz MT, Familiari F, Kennedy NI, et al. Anatomy of the anterior cruciate ligament and the common autograft specimens for anterior cruciate ligament reconstruction. Ann Jt. 2023;8. doi:10.21037/aoj-22-49
- Daniel A V., Smith PA. Primary All-Soft Tissue Quadriceps Tendon Autograft Anterior Cruciate Ligament Reconstruction With Suture Tape Augmentation Resulted in Satisfactory Patient Outcomes and a Low Graft Failure Rate in High School and Collegiate Athletes. Arthroscopy - Journal of Arthroscopic and Related Surgery. Published online January 1, 2024. doi:10.1016/j.arthro.2024.02.047
- Kikuchi N, Kanamori A, Arai N, Okuno K, Yamazaki M. Joint Effusion at 3 Months After Anterior Cruciate Ligament Reconstruction: Its Risk Factors and Association With Subsequent Muscle Strength and Graft Remodeling. Orthop J Sports Med. 2024;12(12). doi:10.1177/23259671241299782
- Ye Z, Chen H, Qiao Y, et al. Intra-Articular Platelet-Rich Plasma Injection after Anterior Cruciate Ligament Reconstruction: A Randomized Clinical Trial. JAMA Netw Open. 2024;7(5):E2410134. doi:10.1001/jamanetworkopen.2024.10134
- Cristiani R, van de Bunt F, Kvist J, Stålman A. High prevalence of associated injuries in anterior cruciate ligament tears: A detailed magnetic resonance imaging analysis of 254 patients. Skeletal Radiol. Published online November 1, 2024. doi:10.1007/s00256-024-04665-9
- D’Ambrosi R R, Sconfienza LM, Albano D, et al. High incidence of RAMP lesions and a nonnegligible incidence of anterolateral ligament and posterior oblique ligament rupture in acute ACL injury. Knee Surgery, Sports Traumatology, Arthroscopy. 2024;32(8):1992-2002. doi:10.1002/ksa.12219
- Saad Berreta R, Villarreal-Espinosa JB, Pallone L, et al. Anterior Cruciate Ligament Repair Results in Similar Patient-Reported Outcome Measures as Anterior Cruciate Ligament Reconstruction: A Systematic Review of Prospective Comparative Studies. Arthroscopy: The Journal of Arthroscopic & Related Surgery. Published online September 2024. doi:10.1016/j.arthro.2024.09.008
- D’Ambrosi R, Carrozzo A, Meena A, et al. A slight degree of osteoarthritis appears to be present after anterior cruciate ligament reconstruction compared with contralateral healthy knees at a minimum of 20 years: A systematic review of the literature. J Exp Orthop. 2024;11(2). doi:10.1002/jeo2.12017
- Cristiani R, van de Bunt F, Kvist J, Stålman A. High Prevalence of Superficial and Deep Medial Collateral Ligament Injuries on Magnetic Resonance Imaging in Patients With Anterior Cruciate Ligament Tears. Arthroscopy - Journal of Arthroscopic and Related Surgery. 2024;40(1):103-110. doi:10.1016/j.arthro.2023.05.029
- Marquez-Lara A, Padget W, Wall EJ, Parikh SN. Predictors and Early Treatment of Knee Arthrofibrosis After Arthroscopic Knee Ligament Reconstruction Surgery in Adolescent Patients. Orthop J Sports Med. 2024;12(12). doi:10.1177/23259671241299838
- Johnson BE, Smith CL, Smith CD, et al. Comparison of Arthrofibrosis After ACL Reconstruction According to Graft Choice: Quadriceps Tendon Versus Bone-Patellar Tendon-Bone Autograft. Orthop J Sports Med. 2025;13(1). doi:10.1177/23259671241311916
- Estevez VM, Danahy P, Whittington J, Ferrell M. How Does a Cyclops Lesion Impact Anterior Cruciate Ligament (ACL) Reconstruction Recovery? Cureus. Published online March 6, 2025. doi:10.7759/cureus.80138
- Tsai YT, Wu CC, Pan RY, Shen PH. Risk Factors for Venous Thromboembolism (VTE) Following Anterior Cruciate Ligament (ACL) reconstruction: A systematic review and meta-analysis. Orthopaedics and Traumatology: Surgery and Research. Published online 2025. doi:10.1016/j.otsr.2025.104184
- Boyd E, Endres NK, Geeslin AG. Postoperative healing and complications based on anterior cruciate ligament reconstruction graft type. Ann Jt. 2024;9:30-30. doi:10.21037/aoj-24-3
- Dave U, Lewis EG, Ierulli VK, Saraf SM, Mulcahey MK. Deep vein thrombosis prophylaxis in patients who undergo knee arthroscopy: a systematic review. Knee Surg Relat Res. 2024;36(1). doi:10.1186/s43019-024-00250-5
- Blumenschein LA, Kolin DA, Fabricant PD, et al. Prevalence of Concomitant Injuries by Sport in Pediatric Patients With ACL Rupture. Orthop J Sports Med. 2024;12(8). doi:10.1177/23259671241260051
- Pruneski JA, Heyworth BE, Kocher MS, et al. Prevalence and Predictors of Concomitant Meniscal and Ligamentous Injuries Associated With ACL Surgery: An Analysis of 20 Years of ACL Reconstruction at a Tertiary Care Children's Hospital. American Journal of Sports Medicine. 2024;52(1):77-86. doi:10.1177/03635465231205556
- Lin YC, Chen YJ, Fan TY, Chou PH, Lu CC. Effect of bone marrow aspiration concentrate and platelet-rich plasma combination in anterior cruciate ligament reconstruction: a randomized, prospective, double-blinded study. J Orthop Surg Res. 2024;19(1). doi:10.1186/s13018-023-04512-y
- Wollenman CC, Cox CL, Schoenecker JG, Wright RW. Venous thromboembolism after Knee Arthroscopy: Incidence, Risk Factors, Prophylaxis, and Management. Journal of the American Academy of Orthopaedic Surgeons. 2024;32(17):e850-e860. doi:10.5435/JAAOS-D-24-00232
- Quesnot A, Mouchel S, Salah S Ben, Baranes I, Martinez L, Billuart F. Randomized controlled trial of compressive cryotherapy versus standard cryotherapy after total knee arthroplasty: pain, swelling, range of motion and functional recovery. BMC Musculoskelet Disord. 2024;25(1). doi:10.1186/s12891-024-07310-7
- Homan MD, Braaten JA, Banovetz MT, Monson JK, Kennedy NI, LaPrade RF. Principles for optimizing anterior cruciate ligament reconstruction outcomes in elite athletes: a review of current techniques. Ann Jt. 2024;9. doi:10.21037/aoj-22-40
- Li Z, Jin L, Chen Z, et al. Effects of Neuromuscular Electrical Stimulation on Quadriceps Femoris Muscle Strength and Knee Joint Function in Patients After ACL Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Orthop J Sports Med. 2025;13(1). doi:10.1177/23259671241275071
- Zhou L, Rothrauff B, Chen L, Jin S, He S, He J. Comparison of blood flow restriction training rehabilitation and general rehabilitation exercise after anterior cruciate ligament reconstruction: A meta-analysis of randomized controlled trials. Knee Surgery, Sports Traumatology, Arthroscopy. Published online 2024. doi:10.1002/ksa.12527
- Rahardja R, Love H, Clatworthy MG, Young SW. Risk factors for reoperation for arthrofibrosis following primary anterior cruciate ligament reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy. 2024;32(3):608-615. doi:10.1002/ksa.12073
- Urhausen AP, Pedersen M, Grindem H, et al. Clinical, Functional, Sports Participation, and Osteoarthritis Outcomes After ACL Injury: Ten-Year Follow-up Study of the Delaware-Oslo ACL Cohort Treatment Algorithm. Journal of Bone and Joint Surgery. Published online April 16, 2025. doi:10.2106/JBJS.24.00243
- Jia Z, Greven J, Hildebrand F, Kobbe P, Eschweiler J. Conservative treatment versus surgical reconstruction for ACL rupture: A systemic review. J Orthop. 2024;57:8-16. doi:10.1016/j.jor.2024.05.026
- Delcogliano M, Sangiorgio A, Bensa A, Andriolo L, Boffa A, Filardo G. Platelet-rich plasma augmentation in anterior cruciate ligament reconstruction: Evidence is still too scattered. A scoping review of randomised controlled trials. Knee Surgery, Sports Traumatology, Arthroscopy. 2024;32(5):1143-1159. doi:10.1002/ksa.12127
- Wong JYS, Ashik MBZ, Mishra N, Lee NKL, Mahadev A, Lam KY. Use of cryotherapy in the postoperative management of paediatric anterior cruciate ligament reconstruction: A prospective randomised controlled trial. Journal of Pediatric Orthopaedics Part B. 2024;33(3):214-222. doi:10.1097/BPB.0000000000001120
- Mayer MA, Deliso M, Hong IS, et al. Rehabilitation and Return to Play Protocols After Anterior Cruciate Ligament Reconstruction in Soccer Players: A Systematic Review. American Journal of Sports Medicine. Published online January 1, 2024. doi:10.1177/03635465241233161
- Butt U, Iqbal J, Shah IA, Khan ZA, Vuletic F, Mohsin A. A comparison of continuous cold flow and compression device and traditional icing regimen and no icing following anterior cruciate ligament reconstruction: A pilot study. J Pak Med Assoc. 2024;74(1):114-117. doi:10.47391/JPMA.7664
- Abd Allah Abd El Hafeez N, Fathy Mohammed Y, Mohammed Z, Khalil Hafez M. Effect of Compressive Cryotherapy on Pain Intensity and Swelling among Patients Post Knee Arthroscopy. Vol 15.; 2024.
- Onobun DE, Orji C, Ojo EO, et al. Exploring the Efficacy of Conservative Management Versus Surgical Intervention in Anterior Cruciate Ligament (ACL) Injuries: Insights Into Reinjury Rates, Quality of Life, and Long-Term Outcomes. Cureus. Published online November 29, 2024. doi:10.7759/cureus.74718
- Moutzouros V, Jildeh TR, Tramer JS, et al. Can We Eliminate Opioids After Anterior Cruciate Ligament Reconstruction? A Prospective, Randomized Controlled Trial. American Journal of Sports Medicine. 2021;49(14):3794-3801. doi:10.1177/03635465211045394
- Jin H, Tahir N, Jiang S, et al. Management of Anterior Cruciate Ligament Injuries in Children and Adolescents: A Systematic Review. Sports Med Open. 2025;11(1). doi:10.1186/s40798-025-00844-7
- Davey MS, Hurley ET, Anil U, et al. Pain Management Strategies After Anterior Cruciate Ligament Reconstruction: A Systematic Review With Network Meta-analysis. Arthroscopy - Journal of Arthroscopic and Related Surgery. 2021;37(4):1290-1300.e6. doi:10.1016/j.arthro.2021.01.023
- Filbay SR, Roemer FW, Lohmander LS, et al. Evidence of ACL healing on MRI following ACL rupture treated with rehabilitation alone may be associated with better patient-reported outcomes: A secondary analysis from the KANON trial. Br J Sports Med. 2022;57(2):91-98. doi:10.1136/bjsports-2022-105473
- Phillips T, Ronna B, Terner Z, Cushing T, Goldenberg N, Shybut T. After 40 days intra-articular injury, risk profile increases linearly with time to surgery in adolescent patients undergoing primary anterior cruciate ligament reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy. Published online April 1, 2024. doi:10.1002/ksa.12423
- Fleming BC, Baranker B, Badger GJ, et al. Bridge-Enhanced Anterior Cruciate Ligament Restoration: 6-Year Results From the First-in-Human Cohort Study. Orthop J Sports Med. 2024;12(8). doi:10.1177/23259671241260632
- Gunadham U, Woratanarat P. Effect of knee bracing on clinical outcomes following anterior cruciate ligament reconstruction: A prospective randomised controlled study. Asia Pac J Sports Med Arthrosc Rehabil Technol. 2024;36:18-23. doi:10.1016/j.asmart.2024.01.006
- Martorell-de Fortuny L, Torres-Claramunt R, Sánchez-Soler JF, Perelli S, Hinarejos P, Monllau JC. Patellar bone defect grafting does not reduce anterior knee pain after bone-patellar tendon-bone anterior cruciate ligament reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy. Published online April 1, 2024. doi:10.1002/ksa.12449
- Devitt BM, Neri T, Fritsch BA. Combined anterolateral complex and anterior cruciate ligament injury: Anatomy, biomechanics, and management - State-of-the-art. Journal of ISAKOS. 2023;8(1):37-46. doi:10.1016/j.jisako.2022.10.004
- Geeslin AG, Moatshe G, Engebretsen L, et al. Functional anterior cruciate ligament braces may have a role in select patient groups although there is presently limited evidence supporting or refuting their routine use: A scoping review of clinical practice guidelines and an updated bracing classification. Knee Surgery, Sports Traumatology, Arthroscopy. 2024;32(7):1690-1699. doi:10.1002/ksa.12203
- Högberg J, Fridh E, Piussi R, et al. Delayed Anterior Cruciate Ligament Reconstruction Is Associated With Lower Odds of Returning to Preinjury Physical Activity Level at 12 Months Follow-Up. Arthroscopy - Journal of Arthroscopic and Related Surgery. Published online 2025. doi:10.1016/j.arthro.2025.02.011
- Kawashima T, Mutsuzaki H, Watanabe A, Ikeda K, Yamanashi Y, Kinugasa T. Impact of Surgical Timing on Functional Outcomes after Anterior Cruciate Ligament Reconstruction. J Clin Med. 2024;13(10). doi:10.3390/jcm13102994
- Musahl V, Nazzal EM, Lucidi GA, et al. Current trends in the anterior cruciate ligament part 1: biology and biomechanics. Knee Surgery, Sports Traumatology, Arthroscopy. 2022;30(1):20-33. doi:10.1007/s00167-021-06826-y
- de Jonge R, Máté M, Kovács N, et al. Nonoperative Treatment as an Option for Isolated Anterior Cruciate Ligament Injury: A Systematic Review and Meta-analysis. Orthop J Sports Med. 2024;12(4). doi:10.1177/23259671241239665
- Kraeutler MJ, Wolsky RM, Vidal AF, Bravman JT. Anatomy and biomechanics of the native and reconstructed anterior cruciate ligament: Surgical implications. Journal of Bone and Joint Surgery - American Volume. 2017;99(5):438-445. doi:10.2106/JBJS.16.00754
- Jensen HA, Nielsen TG, Lind M. Delaying anterior cruciate ligament reconstruction for more than 3 or 6 months results in lower risk of revision surgery. Journal of Orthopaedics and Traumatology. 2024;25(1). doi:10.1186/s10195-024-00759-1
- Jadidi S, Lee AD, Pierko EJ, Choi H, Jones NS. Non-operative Management of Acute Knee Injuries. Curr Rev Musculoskelet Med. 2024;17(1):1-13. doi:10.1007/s12178-023-09875-7
- Glattke KE, Tummala S V., Chhabra A. Anterior Cruciate Ligament Reconstruction Recovery and Rehabilitation: A Systematic Review. Journal of Bone and Joint Surgery. 2022;104(8):739-754. doi:10.2106/JBJS.21.00688
- Babel S, Camporesi E. Efficacy and Safety of Hyperbaric Oxygen Therapy in Ligament and Tendon Injuries: A Systematic Review.
- Stone A V., Marx S, Conley CW. Management of Partial Tears of the Anterior Cruciate Ligament: A Review of the Anatomy, Diagnosis, and Treatment. Journal of the American Academy of Orthopaedic Surgeons. 2021;29(2):60-70. doi:10.5435/JAAOS-D-20-00242
- Holmgren D, Noory S, Moström E, Grindem H, Stålman A, Wörner T. Weaker Quadriceps Muscle Strength With a Quadriceps Tendon Graft Compared With a Patellar or Hamstring Tendon Graft at 7 Months After Anterior Cruciate Ligament Reconstruction. American Journal of Sports Medicine. 2024;52(1):69-76. doi:10.1177/03635465231209442
- Gupta A, Badin D, Lee RJ. The Role of Crutches and Bracing in Preventing Secondary Meniscal Tears After Anterior Cruciate Ligament Injury in Pediatric Patients. Orthop J Sports Med. 2025;13(1). doi:10.1177/23259671241309862
- van Melick N, Senorski EH, Królikowska A, Prill R. Anterior cruciate ligament reconstruction rehabilitation: Decades of change. Knee Surgery, Sports Traumatology, Arthroscopy. Published online April 1, 2025. doi:10.1002/ksa.12600
- D’Ambrosi R, Corona K, Cerciello S, et al. Combining an Anterolateral Complex Procedure With Anterior Cruciate Ligament Reconstruction Reduces Graft Reinjury Without Increasing the Rate of Complications: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Am J Sports Med. Published online January 12, 2025. doi:10.1177/03635465241285887
- Gharpinde MR, Pundkar A, Dhanwani Y, Chandanwale R, Jaiswal AM. Navigating Post-operative Challenges: A Comprehensive Review of Complications Following Anterior Cruciate Ligament (ACL) Tear Surgery. Cureus. Published online August 26, 2024. doi:10.7759/cureus.67768
- Hada S, Hada M, Yoshida K, et al. Conservative Treatment Using Platelet-Rich Plasma for Acute Anterior Cruciate Ligament Injuries in Highly Active Patients: A Retrospective Survey. Cureus. Published online January 28, 2024. doi:10.7759/cureus.53102
- Moiroux-Sahraoui A, Forelli F, Mazeas J, Rambaud AJM, Bjerregaard A, Riera J. Quadriceps Activation After Anterior Cruciate Ligament Reconstruction: The Early Bird Gets the Worm! Int J Sports Phys Ther. 2024;19(8):1044-1051. doi:10.26603/001c.121423
- Lorange JP, Senécal L, Moisan P, Nault ML. Return to Sport After Pediatric Anterior Cruciate Ligament Reconstruction: A Systematic Review of the Criteria. American Journal of Sports Medicine. 2024;52(6):1641-1651. doi:10.1177/03635465231187039
- Özbek EA, Dursun Savran M, Baltacı Ç, et al. Return to Work After Anterior Cruciate Ligament Reconstruction: A Systematic Review. Orthop J Sports Med. 2024;12(5). doi:10.1177/23259671241249086
- Cordasco FA, Hidalgo Perea S, Uppstrom TJ, et al. Quadriceps Tendon Anterior Cruciate Ligament Reconstruction in Skeletally Immature Patients: 3-Year Clinical and Patient-Reported Outcomes. American Journal of Sports Medicine. 2024;52(9):2230-2236. doi:10.1177/03635465241255641
- Kaeding CC, Léger-St-Jean B, Magnussen RA. Epidemiology and Diagnosis of Anterior Cruciate Ligament Injuries. Clin Sports Med. 2017;36(1):1-8. doi:10.1016/j.csm.2016.08.001
- Sánchez M, Yarza I, Jorquera C, et al. Genetics, sex and the use of platelet-rich plasma influence the development of arthrofibrosis after anterior cruciate ligament reconstruction. J Exp Orthop. 2025;12(1). doi:10.1002/jeo2.70156
- Connors JP, Cusano A, Saleet J, et al. Return to Sport and Graft Failure Rates After Primary Anterior Cruciate Ligament Reconstruction With a Bone-Patellar Tendon-Bone Versus Hamstring Tendon Autograft: A Systematic Review and Meta-analysis. American Journal of Sports Medicine. Published online 2025. doi:10.1177/03635465241295713
- Papaleontiou A, Poupard AM, Mahajan UD, Tsantanis P. Conservative vs Surgical Treatment of Anterior Cruciate Ligament Rupture: A Systematic Review. Cureus. Published online March 20, 2024. doi:10.7759/cureus.56532
- Frane N, Bandovic I, Hu V, Bitterman A. Return-to-Driving Recommendations after Lower-Extremity Orthopaedic Procedures. JBJS Rev. 2020;8(12). doi:10.2106/JBJS.RVW.20.00066
- Knapik DM, Singh H, Gursoy S, Trasolini NA, Perry AK, Chahla J. Functional Bracing Following Anterior Cruciate Ligament Reconstruction: A Critical Analysis Review. JBJS Rev. 2021;9(9). doi:10.2106/JBJS.RVW.21.00056
- Carter HM, Littlewood C, Webster KE, Smith BE. The effectiveness of preoperative rehabilitation programmes on postoperative outcomes following anterior cruciate ligament (ACL) reconstruction: A systematic review. BMC Musculoskelet Disord. 2020;21(1). doi:10.1186/s12891-020-03676-6
- BEAR ® Implant Rehabilitation Protocol.
- Golberg E, Sommerfeldt M, Pinkoski A, Dennett L, Beaupre L. Anterior Cruciate Ligament Reconstruction Return-to-Sport Decision-Making: A Scoping Review. Sports Health. 2024;16(1):115-123. doi:10.1177/19417381221147524
- Toth MJ, Tourville TW, Voigt TB, et al. Utility of Neuromuscular Electrical Stimulation to Preserve Quadriceps Muscle Fiber Size and Contractility After Anterior Cruciate Ligament Injuries and Reconstruction: A Randomized, Sham-Controlled, Blinded Trial. American Journal of Sports Medicine. 2020;48(10):2429-2437. doi:10.1177/0363546520933622
- DeFazio MW, Curry EJ, Gustin MJ, et al. Return to Sport After ACL Reconstruction With a BTB Versus Hamstring Tendon Autograft: A Systematic Review and Meta-analysis. Orthop J Sports Med. 2020;8(12). doi:10.1177/2325967120964919
- Cruz AI, Beck JJ, Ellington MD, et al. Failure Rates of Autograft and Allograft ACL Reconstruction in Patients 19 Years of Age and Younger A Systematic Review and Meta-Analysis. JBJS Open Access. 2020;5(4). doi:10.2106/JBJS.OA.20.00106
- Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: The Delaware-Oslo ACL cohort study. Br J Sports Med. 2016;50(13):804-808. doi:10.1136/bjsports-2016-096031
- Marcaccio SE, Morrissey PJ, Testa EJ, Fadale PD. Role of Quadriceps Tendon Autograft in Primary and Revision Anterior Cruciate Ligament Reconstruction. JBJS Rev. 2023;11(10). doi:10.2106/JBJS.RVW.23.00057
- Buerba RA, Zaffagnini S, Kuroda R, Musahl V. ACL reconstruction in the professional or elite athlete: State of the art. Journal of ISAKOS. 2021;6(4):226-236. doi:10.1136/jisakos-2020-000456
- Shah AK, Neijna AG, Retzky JS, Gomoll AH, Strickland SM. Indications, Techniques, and Outcomes of Bridge-Enhanced ACL Restoration (BEAR). Curr Rev Musculoskelet Med. Published online April 1, 2025. doi:10.1007/s12178-025-09950-1
- Failla MJ, Logerstedt DS, Grindem H, et al. Does Extended Preoperative Rehabilitation Influence Outcomes 2 Years after ACL Reconstruction? A Comparative Effectiveness Study between the MOON and Delaware-Oslo ACL Cohorts: American Journal of Sports Medicine. 2016;44(10):2608-2614. doi:10.1177/0363546516652594
- Culvenor AG, Girdwood MA, Juhl CB, et al. Rehabilitation after anterior cruciate ligament and meniscal injuries: A best-evidence synthesis of systematic reviews for the OPTIKNEE consensus. Br J Sports Med. 2022;56(24):1445-1453. doi:10.1136/bjsports-2022-105495
- Anz AW, Branch EA, Jordan SE, et al. Preoperative Platelet-Rich Plasma Injections Decrease Inflammatory and Chondrodegenerative Biomarkers in Patients With Acute Anterior Cruciate Ligament Tears: A Pilot Randomized Controlled Trial. Orthop J Sports Med. 2025;13(3). doi:10.1177/23259671241312754
- Giesche F, Niederer D, Banzer W, Vogt L. Evidence for the effects of prehabilitation before ACL-reconstruction on return to sport-related and self-reported knee function: A systematic review. PLoS One. 2020;15(10 October). doi:10.1371/journal.pone.0240192
- Marois B, Tan XW, Pauyo T, Dodin P, Ballaz L, Nault ML. Can a knee brace prevent ACL reinjury: A systematic review. Int J Environ Res Public Health. 2021;18(14). doi:10.3390/ijerph18147611
- Salem HS, Park DH, Friedman JL, et al. Return to Driving After Anterior Cruciate Ligament Reconstruction: A Systematic Review. Orthop J Sports Med. 2021;9(1). doi:10.1177/2325967120968556
- Wood A, Hargreaves M, Manfredi JN, et al. Anterior Cruciate Ligament Reconstruction Return to Sport Testing Passing Rates for Healthy People: A Systematic Review. American Journal of Sports Medicine. Published online 2025. doi:10.1177/03635465241313194
- Gharpinde MR, Jaiswal AM, Dhanwani Y. A Comprehensive Review of Graft Choices and Surgical Techniques in Primary Anterior Cruciate Ligament Reconstruction: An Outcome Analysis. Cureus. Published online September 5, 2024. doi:10.7759/cureus.68701
- Musahl V, Engler ID, Nazzal EM, et al. Current trends in the anterior cruciate ligament part II: evaluation, surgical technique, prevention, and rehabilitation. Knee Surgery, Sports Traumatology, Arthroscopy. 2022;30(1):34-51. doi:10.1007/s00167-021-06825-z




