What is the clavicle?
The clavicle is commonly referred to as the collar bone. The clavicle attaches the upper extremity to the sternum. Through this connection, the clavicle aids in arm elevation, movement and shoulder strength.

Figure 1 Image showing the bones of the upper extremity with the clavicle labeled. (licensed from Adobe stock)
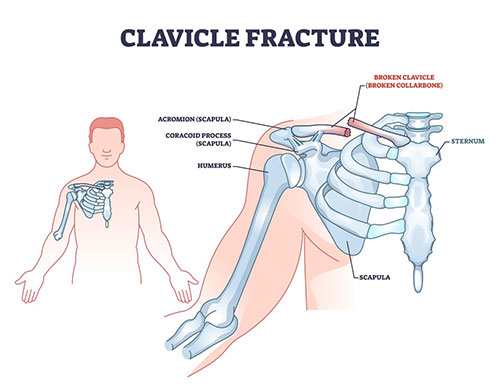
Figure 2 Image demonstrating a clavicle fracture. (licensed from Adobe stock)
How is the clavicle injured?
Fractures of the clavicle occur through both direct and indirect trauma. Clavicle fractures are common in sports such as football, rugby, and soccer. They are also common with motor vehicle accidents or cycling after falls.
What are the symptoms of clavicle fractures?
Fractures of the clavicle will result in pain, swelling and bruising. Displacement of the fracture can result in being able to feel and see the fractured ends of the bone. This is due to the pull of muscles attached to the clavicle.
How is a clavicle fracture diagnosed?
During the clinic visit x-rays will be obtained. This is typically sufficient for diagnosis. In some cases advanced imaging such as MRI or CT scan may be needed for determining more subtle injuries, ruling out related injuries or for surgical planning purposes.

Figure 3 X-ray showing a fractured clavicle.
What are the types of clavicle fractures?
Types of clavicle fracture can largely be grouped based on which area of the clavicle is fractured i.e. medial, middle, or lateral; displacement, and whether or not the clavicle fracture broke through the skin. There are multiple classification systems utilized.
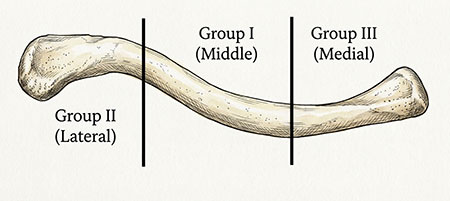
Figure 4 General classification of clavicle fractures
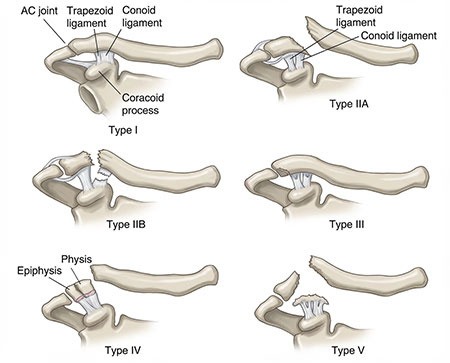
Figure 5 Classification of lateral clavicle fractures
What are the treatment options for clavicle fractures?
Treatment options are always individually tailored. Considerations include age, activity level, type of activity, how recent the injury occurred, location and displacement of the fracture and associated injuries.
The x-rays will be used to evaluate several measurements. Evaluation will include location of the fracture. The most common location of clavicle fractures is the middle third, followed by the lateral aspect of the clavicle. Fractures of the lateral region of the clavicle often have a higher rate of not healing in comparison to fractures of the mid portion of the clavicle.
Other important factors measured on x-rays include the amount of displacement and the amount of shortening of the fractured ends. More displacement and shortening can result in high rates of the bone not healing or lower outcome scores.
Age is an important factor as well. Children and adolescents will often do well without surgery despite displacement and shortening. Some fractures of the lateral end of the clavicle will often do well in older patients even if they do not completely heal.
For non-surgical treatment of the clavicle a sling will be used initially to allow rest of the arm. Patients can typically wean from the sling between 2-6 weeks out from injury. Full healing will still take 3 or more months.
Surgical treatment typically involves placement of one or more plates and screws on the clavicle. For fractures of the mid portion of the clavicle patients are placed in a sling for comfort but are often able to move their shoulder as tolerated after surgery. For fractures of the distal end of the clavicle a sling will be continued for up to 6 weeks to improve healing prior to advancing range of motion.
How is clavicle fracture fixation performed?
The surgery is performed under a general anesthetic typically with the use of a regional nerve block.
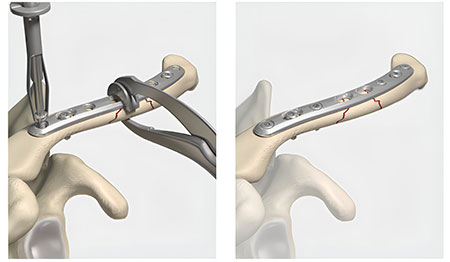
Figure 6 After an incision is made, the fracture is exposed and reduced using clamps. A metal plate is then placed and then secured with screws. (credit: Arthrex.com)
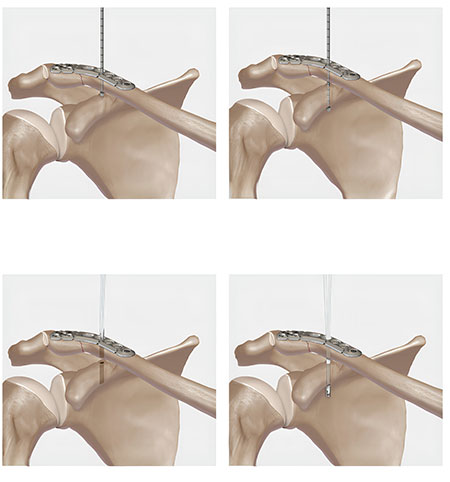
Figure 7 If injury to the ligaments connecting to clavicle to the coracoid has occured, a device such as the one noted above may be used the secure the clavicle and the plate to the coracoid. This can be done through the same incision. (credit: Arthrex.com)
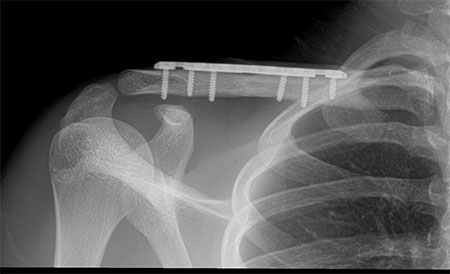
Figure 8 Example of a clavicle after surgical fixation.
Timing of clavicle surgery
Surgery is ideally performed within 2-3 weeks from the time of injury. Although surgery can be performed after this time period it may require additional procedures such as osteotomy (re-breaking the bone) in order to properly reduce the fracture.
Outcomes of clavicle fracture surgery
Outcomes after clavicle surgery are generally good to excellent. The majority of patients are able to return to their pre injury activity level. Bony healing is typically achieved by 3-4 months after surgery.
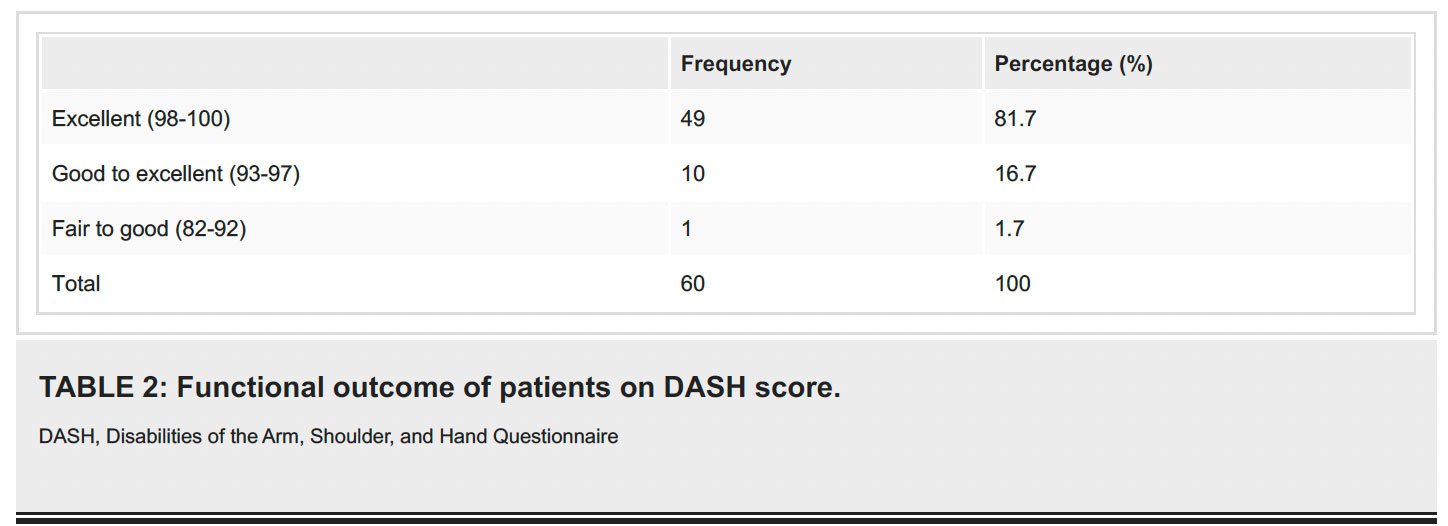
Figure 9 Outcome table from 2024 Mannan et al. Cureus 16(10): e72048. DOI 10.7759/cureus.72048
Return to sport after clavicle fracture surgery
The majority of patients are able to return to sport after clavicle fracture surgery with many studies reporting rates from 80-100% return to sport. Timing of return to sport will largely depending on patient age, type and level of sport. In general, timing for return to sport is often expected at 6-16 weeks after surgery.
What are the possible complications after clavicle fracture surgery?
Complication rates after surgical fixation have been reported around 5-30%.
Infection
Infection is an uncommon complication after this type of surgery. Rates are typically below 3% for any type of infection with rates of deep infection being less than 1%. Smoking can increase infection risk. Prevention at the time of surgery includes the surgical sterilization of the skin and using the use of antibiotics at the time of surgery. Presentation of infections could include fever, chills, increased pain and swelling at the surgical site, redness, warmth and drainage. Management often includes antibiotics and possibly surgical irrigation and debridement and possible removal of the hardware.
Nerve Injury
Major nerve injury is uncommon. Delayed time to surgery can increase the chance of nerve injury secondary to adhesions formed between the fracture and brachial plexus. More common nerve injury involves the suprascapular nerves. These nerves provide sensation to the upper chest. It is more common to have an injury these nerves at the time of surgery. This may result in a numb area at the chest.
Vascular Injury
Major vascular injury is rare. Injuries could include vessel injury, arterio-venous fistula, deep venous thrombosis, or pseudoaneurysm. Reports of these injuries are typically < 1%. Treatment of these injuries would be on a case by case basis.
Malunion and nonunion
Malunion is when the bone heals in the incorrect position. Nonunion is when the bone does not heal at all. Both appear to occur at rates < 4%. Treatment of malunions may not always be required beyond normal recovery as some patients remain asymptomatic. If symptoms persist, treatment may include revision surgery to correct bony alignment. In the case of nonunion, treatment may include treatment of underlying causes for the nonunion, including smoking cessation, correction of vitamin D levels, use of a bone stimulator or possible revision surgery.
Hardware irritation
Hardware irritation is the most common reason for reoperation after clavicle fracture surgery. Due to the hardware location there can be irritation in the region. If this pain persists after bone healing a second surgery may be required to remove the hardware.
Other reported complications
Other complications reported include, shoulder stiffness, hardware breakage, delayed union, shoulder weakness and continued pain.
This is not an exhaustive list of all complications. Other complications, although uncommon, can still occur.
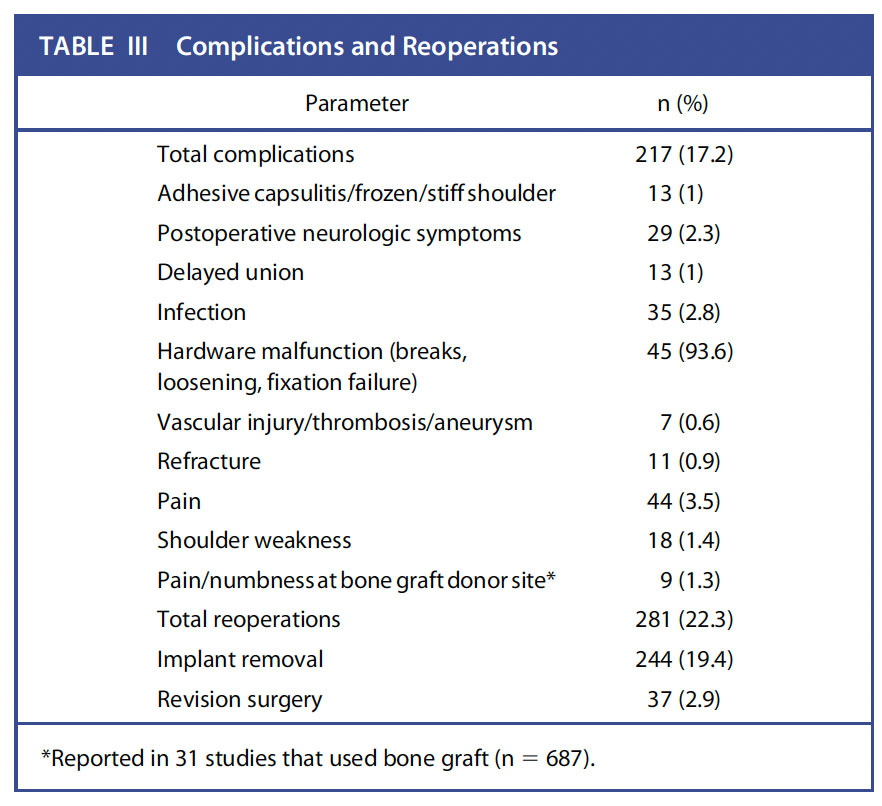
Figure 10 Complication tables from JBJS REVIEWS 2023;11(1):e22.00171 · http://dx.doi.org/10.2106/JBJS.RVW.22.00171
Pain management after surgery
Narcotic pain medications and anti inflammatories may be prescribed after surgery to help reduce pain. Nerve blocks at the time of surgery have been shown to be affective at reducing pain with low risk of long term deficits.
Do I need to use a sling after my clavicle fracture surgery?
Patients will be placed in a sling post operatively. You will use this sling for comfort but are able to come out of the sling as symptoms allow.
When can I return to work after surgery?
Return to work will largely depend on your specific occupational requirements. Many patients are no longer requiring the use of pain medications during the day by the third to fifth day after surgery. If your work is sedentary, you may be able to return as soon as this time. Work that involves heavy lifting will require longer periods away from work if light duty is not available.
When can I drive after surgery?
There is no definitive test we can do to determine when a patient is safe to return to driving. You should not be taking narcotic or sedating medications prior to driving. You should also not need the use of a sling. In general, a patient should possess the strength and range of motion to utilize the vehicles steering wheel in all situations prior to driving.
Post operative Instructions
- Following your stay in the recovery room and when your vital signs are stable you will be discharged to your escort.
- Remember, it is normal to feel a little dizzy or drowsy for several hours after surgery. This is due to the action the medicine used during surgery.
- If you do not have a post operative appointment scheduled, please call the office as soon as possible to schedule this appointment.
- Take your pain medicine as directed. Begin the pain medicine before you start getting uncomfortable, as the nerve block will wear off. If you wait to take your pain medication until the pain is severe, you will have more difficulty in controlling the pain.
- If you are taking narcotic pain medication you may need a stool softener to prevent constipation. Over-the-counter medication such as Docusate or Milk of Magnesia is recommended.
- Notify the office of any fever, chills, or temperature > 100.5.
- Notify the office of any wound drainage.
Post-Surgery Diet
- Resume your diet as tolerated and include vegetables, fruits, and proteins (such as meats, fish, chicken, nuts, and eggs) to promote healing. Also, remember to have adequate fluid intake. It is common after surgery to lack an appetite. This may be the result of anesthesia and the medications. Proper nutrition is needed for healing. During the healing process, the body needs increased amounts of calories and protein. Eat a variety of foods to get all the calories, proteins, vitamins, and minerals you need. If you have been told to follow a specific diet, please follow it.
How should I manage my surgical site and bandages?
Your incision is typically closed with buried dissolvable sutures covered by a skin glue. This will be covered with a bandage after surgery. This bandage can be removed on the second day after surgery. You are able to shower after removing the bandage.
What is my activity level after surgery?
You will use a sling for comfort. It is okay to remove the sling as tolerated and move the elbow. You should not be lifting with the shoulder. You are also encouraged to move your fingers as tolerated. Elevation of the hand will aid with swelling.
Can I smoke following surgery?
You should not smoke after surgery as it interferes with healing.
Questions or Concerns
If at anytime you have questions or concerns you can either contact your surgeon’s medical assistant via email or you can call the main office numbers at: (855) 624-3306. You can also use the electronic medical record’s online portal to send questions.
Example rehabilitation protocol:
Sling for 4-10 days (FOR COMFORT ONLY)
- Post-OP Week 0-1:
- Begin:
- Goals:
- 1. Minimize pain and inflammation
2. Full elbow and wrist ROM
3. Scapular stabilization
4. No active shoulder ROM, lifting, supporting body weight or lifting of body weight with hands - Exercises Days 1-10:
- 1. Pendulum SWINGS
2. Squeeze ball - Post-OP Weeks 2-4:
- Begin:
- Exercises:
- 1. Pendulums to warm up
2. Active ROM with passive stretching
3. Gentle pulley for shoulder
4. Isometric scapular PNF - Post-OP Weeks 4-8:
- Begin:
- Goals:
- 1. Pendulums to warm up and con't with phase 2
2. Begin resistance exercises
3. May begin lifting 5 lbs (ONLY AFTER 6 WEEKS)
4. May begin elliptical without active arm movement
5. Continue NWB UE - Exercises:
- 1. Mid-range motion of rotator cuff (ER and IR rotations)
2. Active and light resistance exercises (through 75% of ROM as patient's symptoms permit) without shoulder elevation and extreme end ROM
3. Strive for progressive gains to active 90° of shoulder flexion and abduction
4. Shrugs, seated rows, etc - Post-OP Weeks 8-12:
- Begin:
- Goals:
- 1. Maintain full pain-free ROM
2. Increase manual mobilizations of soft tissue as well as GHJ and scapulothoracic jts for ROM
3. No repeated heavy resisted exercises or lifting until 3 months
Golf: 8 weeks, chip/putt only Tennis: 3 months Contact Sports: 4 months (per MD clearance)
References:
- von Rüden C, Rehme-Röhrl J, Augat P, et al. Evidence on treatment of clavicle fractures. Injury. 2023;54. doi:10.1016/j.injury.2023.05.049
- Kilkenny CJ, Daly GR, Whelehan SP, et al. Return to play following clavicular fracture – A systematic review and meta analysis. JSES Reviews, Reports, and Techniques. Elsevier Inc. 2025;5(2):259-269. doi:10.1016/j.xrrt.2024.11.002
- Ropars M, Thomazeau H, Huten D. Clavicle fractures. Orthopaedics and Traumatology: Surgery and Research. Elsevier Masson SAS. 2017;103(1):S53-S59. doi:10.1016/j.otsr.2016.11.007
- Baxendale-Smith LD, Teed R, Nicholson JA. Adolescent displaced lateral-end clavicle fractures are not comparable to the adult variant. Epidemiology, fracture patterns and outcome of non-operative management. Shoulder Elbow. 2023;15(6):619-625. doi:10.1177/17585732221131922
- Annicchiarico N, Latta A, Santolini E. Plate osteosynthesis for mid-shaft clavicle fractures: An update. Injury. 2023;54:S53-S57. doi:10.1016/j.injury.2020.10.085
- Wurm M, Zyskowski M, Pesch S, Biberthaler P, Kirchhoff C, Beirer M. Good to excellent functional outcome and high return to sports rate after operative treatment of unstable lateral clavicle fractures: Comparison of two coracoclavicular button fixation techniques. J Clin Med. 2021;10(20). doi:10.3390/jcm10204685
- Yang S, Andras L. Clavicle Shaft Fractures in Adolescents. Orthopedic Clinics of North America. W.B. Saunders. 2017;48(1):47-58. doi:10.1016/j.ocl.2016.08.007
- Woltz S, Krijnen P, Schipper IB. Plate fixation versus nonoperative treatment for displaced midshaft clavicular fractures: A meta-analysis of randomized controlled trials. Journal of Bone and Joint Surgery - American Volume. Lippincott Williams and Wilkins. 2017;99(12):1051-1057. doi:10.2106/JBJS.16.01068
- Heyworth BE, Pennock AT, Li Y, et al. Two-Year Functional Outcomes of Operative vs Nonoperative Treatment of Completely Displaced Midshaft Clavicle Fractures in Adolescents: Results From the Prospective Multicenter FACTS Study Group. American Journal of Sports Medicine. 2022;50(11):3045-3055. doi:10.1177/03635465221114420
- Matsubara Y, Nakamura Y, Sasashige Y, Yokoya S, Adachi N. Long-term conservative treatment outcomes for midshaft clavicle fractures: a 10-to-30-year follow-up. J Orthop Surg Res. 2023;18(1). doi:10.1186/s13018-023-04450-9
- Yadav S, Phalak MO, Shevate I, et al. Comparative Study of Postoperative Outcomes of Clavicle Midshaft Fracture Treated by Nailing vs. Plating. Cureus. Published online March 5, 2022. doi:10.7759/cureus.22862
- Ryan DJ, Iofin N, Furgiuele D, Johnson J, Egol K. Regional anesthesia for clavicle fracture surgery is safe and effective. J Shoulder Elbow Surg. 2021;30(7):e356-e360. doi:10.1016/j.jse.2020.10.009
- Gobbell W, Edwards CM, Engel SR, Coyner KJ. Getting Athletes Back on the Field: Management of Clavicle Fractures and Return to Play. Clin Sports Med. W.B. Saunders. 2023;42(4):649-661. doi:10.1016/j.csm.2023.05.006
- Kihlström C, Möller M, Lönn K, Wolf O. Clavicle fractures: epidemiology, classification and treatment of 2 422 fractures in the Swedish Fracture Register; an observational study. BMC Musculoskelet Disord. 2017;18(1). doi:10.1186/s12891-017-1444-1
- Lima GV, La Banca V, Murachovsky J, Nascimento LGP, Almeida LHO, Ikemoto RY. Assessment of the measurement methods in midshaft clavicle fracture. BMC Musculoskelet Disord. 2022;23(1). doi:10.1186/s12891-022-05961-y
- Hornung CM, Kramer R, Levine J, Hannink G, Hoogervorst P. Functional outcomes and complications of plate fixation for midshaft clavicle fractures by type and location: a systematic review and meta-analysis. JSES Int. Elsevier B.V. 2024;8(3):407-422. doi:10.1016/j.jseint.2024.01.007
- Pradel S, Brunaud M, Coulomb R, Kouyoumdjian P, Marès O. Less than 1.5 cm shortening in clavicle midshaft fracture has long-term functional impact. Orthopaedics and Traumatology: Surgery and Research. 2023;109(5). doi:10.1016/j.otsr.2023.103590
- Hu R, Su YJ, Chien CS. Supraclavicular nerve sparing versus sacrifice during open reduction internal fixation of acute midshaft clavicle fracture. J Orthop Surg Res. 2023;18(1). doi:10.1186/s13018-023-04220-7
- Patel M, Heyworth BE, Dehghan N, Mehlman CT, McKee MD. Clavicular Fractures in the Adolescent. Journal of Bone and Joint Surgery. 2023;105(9):713-723. doi:10.2106/JBJS.22.01036
- Sharma A, Shaffrey I, Reiter CR, et al. Risk factors for adverse events after clavicle fracture open reduction and internal fixation: A NSQIP study. Injury. 2024;55(11). doi:10.1016/j.injury.2024.111883
- Polinsky SG, Edmonds EW, Bastrom TP, et al. 5-Year Radiographic and Functional Outcomes of Nonoperative Treatment of Completely Displaced Midshaft Clavicular Fractures in Teenagers. American Journal of Sports Medicine. 2024;52(4):1032-1039. doi:10.1177/03635465241228818
- Wolf S, Chitnis AS, Manoranjith A, et al. Surgical treatment, complications, reoperations, and healthcare costs among patients with clavicle fracture in England. BMC Musculoskelet Disord. 2022;23(1). doi:10.1186/s12891-022-05075-5
- Ankers T, Sawalha S, Nixon M, Kenyon P, Webb M. Does a skin incision along Langer’s lines reduce complications following fixation of displaced middle-third clavicle fractures? Arch Orthop Trauma Surg. 2022;142(6):1003-1007. doi:10.1007/s00402-021-03766-7
- Yang TH, Ko HJ, Wang AD, et al. Complications of clavicle fracture surgery in patients with concomitant chest wall injury: a retrospective study. BMC Musculoskelet Disord. 2021;22(1). doi:10.1186/s12891-021-04148-1
- Willimon SC, Wilson PL, Quinn M, et al. Completely Displaced Midshaft Clavicular Fractures with Skin Tenting in Adolescents Results from the FACTS Multicenter Prospective Cohort Study. Journal of Bone and Joint Surgery. 2025;107(14):1553-1560. doi:10.2106/JBJS.24.00083
- Sliepen J, Hoekstra H, Onsea J, et al. Treatment and outcome of fracture-related infection of the clavicle. Injury. 2023;54(8). doi:10.1016/j.injury.2023.110910
- Yetter T, Harper J, Weatherby PJ, Somerson JS. Complications and Outcomes After Surgical Intervention in Clavicular Nonunion: A Systematic Review. JBJS Rev. Journal of Bone and Joint Surgery Inc. 2023;11(1). doi:10.2106/JBJS.RVW.22.00171
- Ahearn BM, Shanley E, Thigpen CA, Pill SG, Kissenberth MJ. Factors influencing time to return to sport following clavicular fractures in adolescent athletes. J Shoulder Elbow Surg. 2021;30(7):S140-S144. doi:10.1016/j.jse.2021.04.006
- Trivellas M, Wittstein J. Midshaft Clavicle Fractures: When Is Surgical Management Indicated and Which Fixation Method Should Be Used? Clin Sports Med. W.B. Saunders. 2023;42(4):633-647. doi:10.1016/j.csm.2023.05.005
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. BMJ Publishing Group. 2021;372. doi:10.1136/bmj.n71
- Zheng Y, Li J, Tam AYC, et al. Finite element modeling of clavicle fracture fixations: a systematic scoping review. Med Biol Eng Comput. Springer Science and Business Media Deutschland GmbH. 2025;63(6):1585-1607. doi:10.1007/s11517-025-03294-1
- Spence DD, Wilson PL, Pennock AT, et al. Treatment of Severely Shortened or Comminuted Clavicular Fractures in Older Adolescent Athletes. American Journal of Sports Medicine. 2024;52(2):423-430. doi:10.1177/03635465231219248
- Sheth MM, Shybut TB. Operative Management for Displaced Distal Clavicle Fractures. Clin Sports Med. W.B. Saunders. 2023;42(4):695-711. doi:10.1016/j.csm.2023.06.017
- Ahrens PM, Garlick NI, Barber J, Tims EM. The Clavicle Trial. Journal of Bone and Joint Surgery - American Volume. 2017;99(16):1345-1354. doi:10.2106/JBJS.16.01112
- Baertl S, Alt V, Rupp M. Surgical enhancement of fracture healing – operative vs. nonoperative treatment. Injury. 2021;52:S12-S17. doi:10.1016/j.injury.2020.11.049
- Smith JR, Kitzen J, Buckley R. Midshaft clavicle fracture – Nonoperative versus operative care. Injury. Elsevier Ltd. 2021;52(8):2049-2051. doi:10.1016/j.injury.2020.11.066
- Scott ML, Baldwin KD, Justin Mistovich R. Operative Versus Nonoperative Treatment of Pediatric and Adolescent Clavicular Fractures: A Systematic Review and Critical Analysis. JBJS Rev. 2019;7(3). doi:10.2106/JBJS.RVW.18.00043
- Asadollahi S, Bucknill A. Acute medial clavicle fracture in adults: a systematic review of demographics, clinical features and treatment outcomes in 220 patients. Journal of Orthopaedics and Traumatology. Springer-Verlag Italia s.r.l. 2019;20(1). doi:10.1186/s10195-019-0533-3
- Maheshwari P, Peshin C, Agarwal D. Functional Outcomes in Surgically Treated Clavicle Fractures: A Longitudinal Observational Study. Cureus. Published online November 1, 2023. doi:10.7759/cureus.48081
- Burnham JM, Kim DC, Kamineni S. Midshaft clavicle fractures: A critical review. Orthopedics. Slack Incorporated. 2016;39(5):e814-e821. doi:10.3928/01477447-20160517-06
- Lian J, Chan FJ, Levy BJ. Classification of Distal Clavicle Fractures and Indications for Conservative Treatment. Clin Sports Med. W.B. Saunders. 2023;42(4):685-693. doi:10.1016/j.csm.2023.05.007
- Oberle L, Pierpoint L, Spittler J, Khodaee M. Epidemiology of Clavicle Fractures Sustained at a Colorado Ski Resort. Orthop J Sports Med. 2021;9(5). doi:10.1177/23259671211006722
- Konarski A, Walmsley M, Jain N. Return to competition following clavicle fractures in professional road cyclists. J Orthop. 2022;34:100-103. doi:10.1016/j.jor.2022.08.009
- Fourman MS. CORR Insights®: Minimal Pain Decrease between 2 and 4 Weeks after Nonoperative Management of a Displaced Midshaft Clavicle Fracture Is Associated with a High Risk of Symptomatic Nonunion. Clin Orthop Relat Res. Lippincott Williams and Wilkins. 2021;479(1):139-141. doi:10.1097/CORR.0000000000001606
- Charles SJC, Chen SR, Mittwede P, et al. Risk factors for complications and reoperation following operative management of displaced midshaft clavicle fractures. J Shoulder Elbow Surg. 2022;31(10):e498-e506. doi:10.1016/j.jse.2022.03.016
- Borole A, Vitkovska D, Yang J, Avendano JP, Monica J, Katt BM. Neurovascular Complications Following Clavicle Fracture Fixation: Timing, Mechanisms, and Clinical Implications. Cureus. Published online November 26, 2024. doi:10.7759/cureus.74512
- Mannan M, Hafeez U, Hassan A, Tahir R, Ajnin S. Functional Outcomes of Clavicle Open Reduction and Internal Fixation (ORIF). Cureus. Published online October 21, 2024. doi:10.7759/cureus.72048
- Varady NH, Jones RH, Bram JT, Seeley MA, Fabricant PD. Safety of Accelerated Return to Play After Anatomic Open Reduction and Internal Fixation of Adolescent Clavicle Fractures. Orthop J Sports Med. 2025;13(9). doi:10.1177/23259671251374299




