https://pubmed.ncbi.nlm.nih.gov/33797979/
Today’s article is “Clinical Outcome of a Modified Coracoid Tunnel-Free Coracoclavicular Sling Technique With Remnant Preservation for the Treatment of High-Grade Acromioclavicular Joint Separation: A Report of 48 Cases With 2 to 5 Years of Follow-up”. This study from Li et al. was performed at Beijing Jishuitan Hospital, Beijing, China.
I like this study as I think the topic is interesting. Shoulder separations are frequently in the news with football players. In my practice most of these injuries are from football or falls from a bicycle but can also occur during other sporting activities, falls, or car accidents.
The acromioclavicular joint (AC joint) is stabilized by the coracoclavicular and acromioclavicular ligaments. This study focuses on grade 4 and 5 AC joint separations. Briefly, these injuries are graded by degree and direction of displacement of the clavicle in relation to the acromion. A type 4 separation results in a distal clavicle that is displaced posterior in relation to the acromion. A type 5 separation results in a superiorly displaced distal clavicle of greater than 100%.
The authors describe a technique that uses two drill holes in the clavicle with passage of suture under the coracoid and secured with two buttons on the superior surface of the clavicle with an adjustable suture. One of the worries with type of technique is that the suture can act as a saw under the coracoid and result in fractures. The authors did not have this complication during their follow up period. The authors also mention a desire to limit techniques requiring tunnels in the coracoid itself as this can also result in coracoid complications especially in their small statured patient population.
The results from the study are promising with 41 of 48 returning to preinjury level of sporting activity although they do not explicitly state either the level of or type of sport. They showed a loss of reduction rate of 8.3% but this did not require further intervention.
There is no shortage of different techniques to treat this condition. My current technique is a modification of one described by Menge et al. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5368056/
I have included a very rough illustration of the author’s described technique. You can also watch the patient education videos for further info.
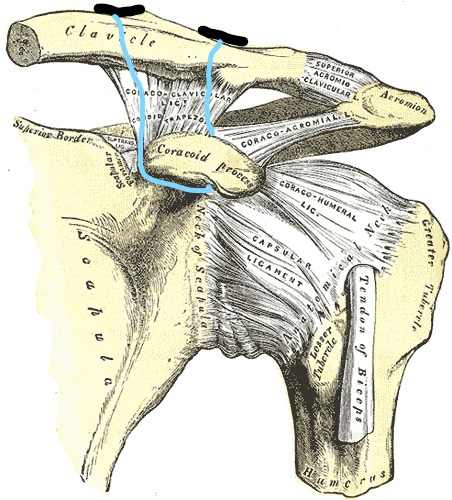
Fig. 1- Two buttons can be seen on the superior surface of the clavicle. The suture connecting the two buttons is adjustable and serves to reduce the injury.
If you are suffering from pain and discomfort following acromioclavicular joint separation and want to discuss more about the treatment options, call my office at 512-244-4272 or schedule an appointment online.




