What is the distal radius?
The radius is one of the bones of the forearm. It extends from the elbow to the wrist. The distal end refers to the portion of the bone closest to the wrist. The radius is involved with the motions of the elbow, including flexion and extension. It is also involved wrist flexion, extension, radial and ulnar deviation as well as forearm rotation (supination and pronation).
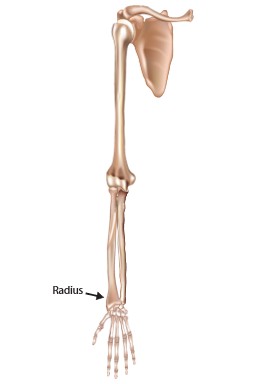
Figure 1. Bone of the upper extremity with the arrow pointing to radius. (Licensed from Adobe stock)
How is the distal radius injured?
The radius is commonly injured during a fall onto an outstretched hand. Other common causes include car accidents or injuries during sporting activities.
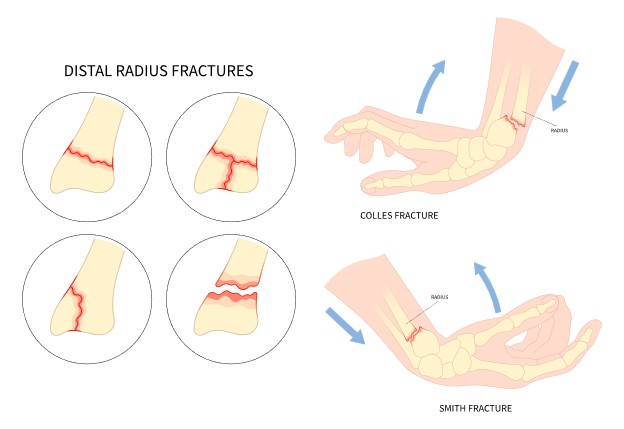
Figure 2. Image demonstrating fall on to hand resulting in a distal radius fracture. Other fracture types also demonstrated. (Licensed from Adobe stock)
What are the symptoms of distal radius fractures?
The most common symptoms of distal radius fractures are pain and swelling at the wrist. Pain is typically worsened with wrist motion. There can also be an obvious deformity of the wrist if the fracture is very displaced.
How is a distal radius fracture diagnosed?
During the clinic visit x-rays will be obtained. This is typically sufficient for diagnosis. In some cases advanced imaging such as MRI or CT scan may be needed for determining more subtle injuries, ruling out related injuries or for surgical planning purposes.

Figure 3. X-rays demonstrated a wrist without fracture on the top row and x-rays showing a fracture on the bottom row.
What are the treatment options for distal radius fractures?
Treatment options are always individually tailored. Considerations include age, activity level, type of activity, how recent the injury occurred, partial versus complete tear, prior treatment, and associated injuries.
The x-rays will be used to evaluate several measurements. One of the more important measurements is the dorsal tilt. See figure for an example of measurements. Certain fracture types also tend to be more unstable and have better outcomes with surgical fixation.
For non surgical treatment of distal radius fractures splint and/or cast immobilization is utilized for 4-8 weeks. Immobilization may include either short or long arm splints/casts. The type and duration of immobilization with depend on patient age, activity, level and fracture instability.
Surgical treatment typically involves the placement of a plate and screws on the radius. This will typically hold the fracture stable to allow for early range of motion. After fixation of the wrist, range of motion is typically started within 7-14 days. This allows for earlier return to full range of motion and independence. In cases where other injuries are present or in very unstable fracture patterns a fixation method known as bridge plating may be used. This involves placing a plate across the wrist with screws in the hand (metacarpal) and forearm (radius). Due to the nature of the plating method, early range of motion is not performed. This also requires a second surgery for plate removal to allow for range of motion of the wrist.
How is distal radius fixation performed?
The surgery is performed under a general anesthetic typically with the use of a regional nerve block.
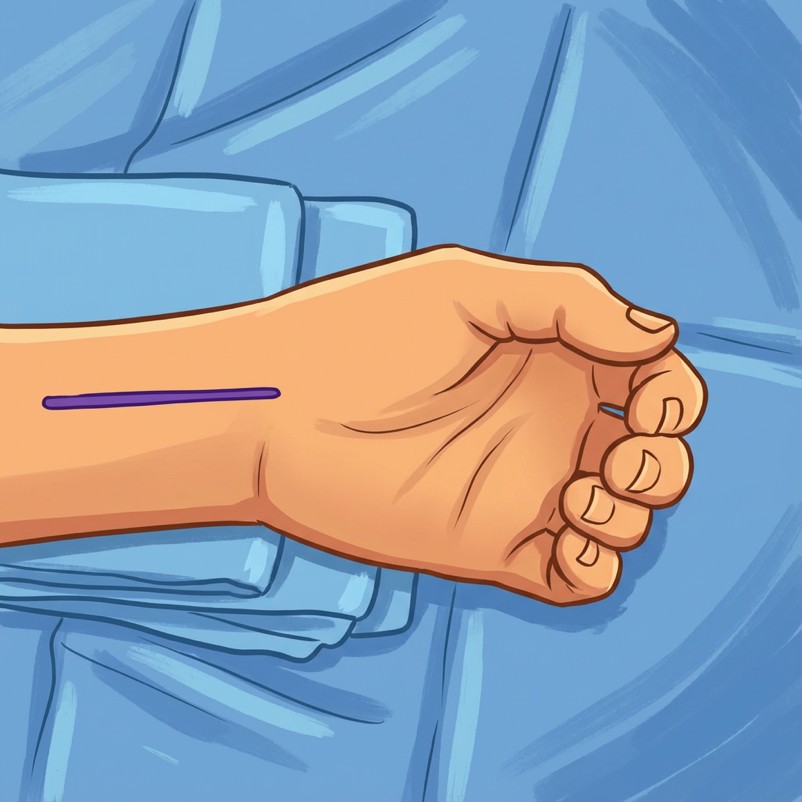
Figure 4. A roughly 6-8 centimeter incision is made over the wrist where the purple line is shown above.
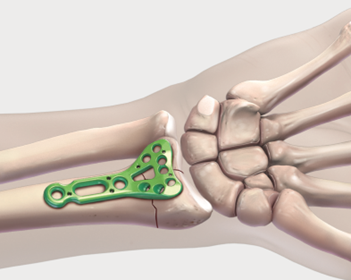
Figure 5. The fracture is then identified, reduced, and the plate is placed in an appropriate position. (credit: Arthrex.com)
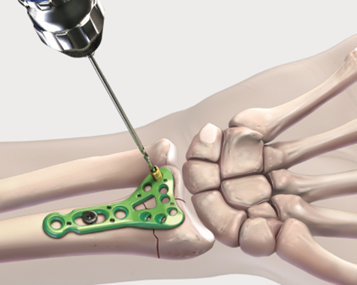
Figure 6. Once reduction is achieved, screws are then placed to hold the fracture in place. (credit: Arthrex.com)
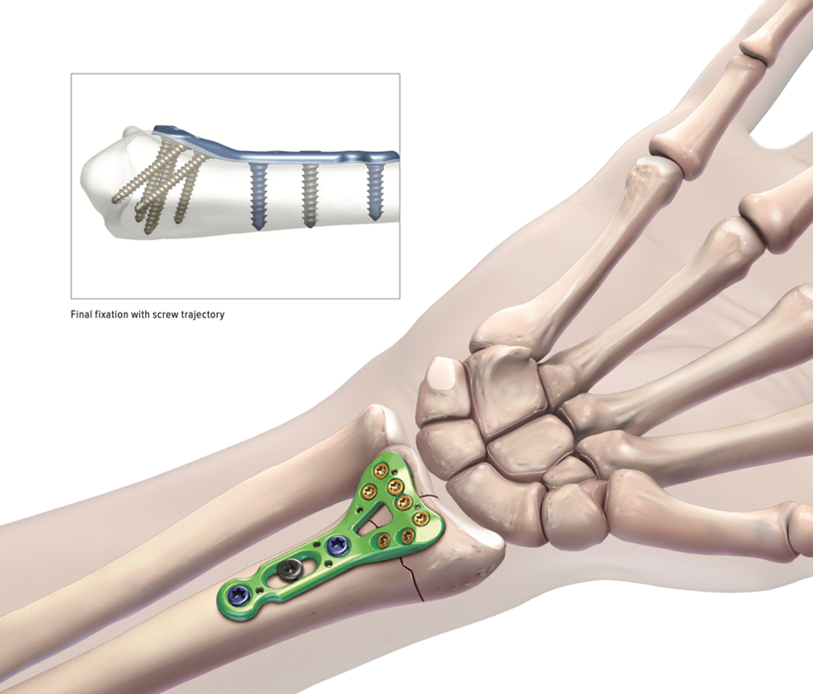
Figure 7. Example of an x-ray in the top left showing the screws in place. (credit: Arthrex.com)
Timing of distal radius surgery
Surgery is ideally performed within 2-3 weeks from the time of injury. Although surgery can be performed after this time period it may require additional procedures such as osteotomy (re-breaking the bone) in order to properly reduce the fracture.
Outcomes of distal radius surgery
Outcomes following distal radius surgery are generally good. Grip strength has been found in studies to return to ~70-100% of the uninjured side. Patient reported outcome measures typically show the greatest improvement in the first 3-6 months following surgery with additional, progressive, improvement extending to 1 year and beyond.
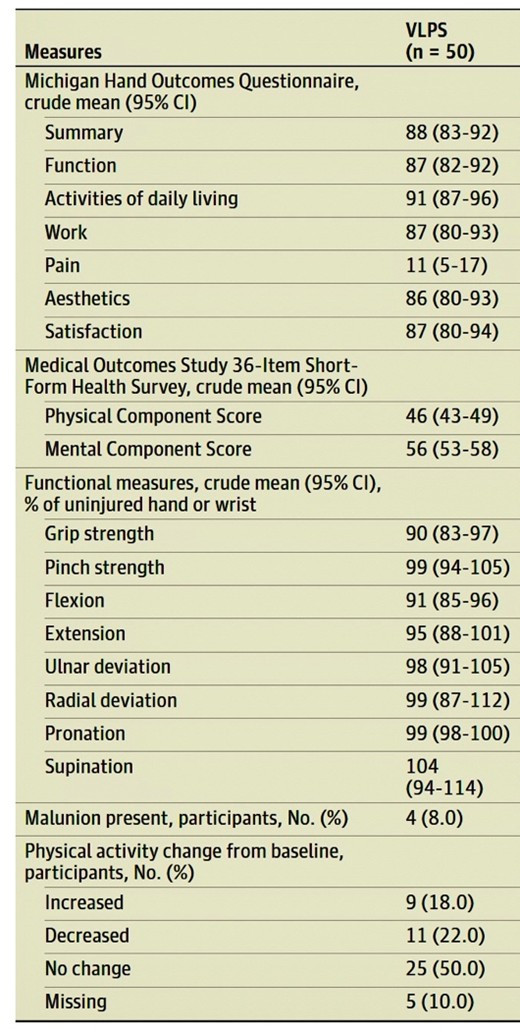
Figure 8. Table summarizing outcomes from "Comparison of 24-Month Outcomes After Treatmetn for Distal Radius Fracture The WRIST Randomzed Clinical Trial" JAMA Network Open. 2021;4(6):e2112710. (VLPS- Volar locking plate system)
Return to sport after distal radius surgery
There are currently no generally accepted guidelines on return to sport. In general, return to sport will be determined based on the specific sport, position, and activity level. You should typically have achieved a pain free range of motion with xray evidence of fracture healing prior to return.
What are the possible complications after distal radius surgery?
Complication rates after surgical fixation have been reported around 5-30%.
Infection
Infection is an uncommon complication after this type of surgery. Rates are typically below 3% for any type of infection with rates of deep infection being less than 1%. Smoking can increase infection risk. Prevention at the time of surgery includes the surgical sterilization of the skin and using the use of antibiotics at the time of surgery. Presentation of infections could include fever, chills, increased pain and swelling at the surgical site, redness, warmth and drainage. Management often includes antibiotics and possibly surgical irrigation and debridement.
Nerve Injury
Major nerve injury is uncommon. Carpal tunnel syndrome can be associated with the trauma of the fracture itself. In some cases a carpal tunnel release may be performed at the time of fracture fixation. Peri-incisional numbness can also occur. This can result in an area of decreased sensation and can occur in <10% of cases. This typically resolves with observation.
Vascular Injury
Injury to the radial artery has been reported but is extremely rare. Injury to this artery may require a vascular repair.
Tendon injury
Irritation and rupture of both flexor and extensor tendons at the wrist can occur. Although irritation may occur in up to 5% of patients, rupture is typically seen in <1% of cases. If irritation is persistent this may require removal of hardware that is irritating the tendon. In cases of rupture this may require tendon repair or tendon transfer.
Malunion and nonunion
Malunion is when the bone heals in the incorrect position. Nonunion is when the bone does not heal at all. Both appear to occur at rates < 4%. Treatment of malunions may not always be required beyond normal recovery as some patients remain asymptomatic. If symptoms persist, treatment may include revision surgery to correct bony alignment. In the case of nonunion, treatment may include treatment of underlying causes for the nonunion, including smoking cessation, correction of vitamin D levels, use of a bone stimulator or possible revision surgery.
Other reported complications
Other reported complications include wrist stiffness, radius fracture, complex regional pain syndrome and compartment syndrome.
This is not an exhaustive list of all complications. Other complications, although uncommon, can still occur.
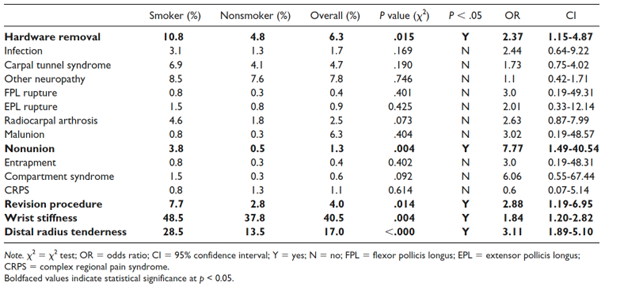
Figure 9. Table summarizing outcomes from "Smoking Increases Postoperative Complications After Distal Radius Fracture Fixation: A review of 417 Patients From a Level 1 Trauma Center" Hand 2020, Vol.15(5) 686-691.
Pain management after surgery
Medications including narcotic pain medications and anti inflammatories may be prescribed after surgery to help reduce pain. Nerve blocks at the time of surgery have been shown to be affective at reducing pain with low risk of long term deficits.
Do I need to use a brace after my distal radius fracture surgery?
Most patients will be placed in a short arm splint immediately following surgery. Patients will then be transitioned to a removable wrist brace between 1-2 weeks after surgery. This can then be removed as tolerated to begin range of motion. Less commonly a long arm splint may be utilized after surgery. In these cases, transition to a brace will be dependent on the stability of the fracture.
When can I return to work after surgery?
Return to work will largely depend on your specific occupational requirements. Many patients are no longer requiring the use of pain medications during the day by the third to fifth day after surgery. If your work is sedentary, you may be able to return as soon as this time. Work that involves heavy lifting may require longer periods away from work if light duty is not available.
When can I drive after surgery?
There is no definitive test we can do to determine when a patient is safe to return to driving. You should not be taking narcotic or sedating medications prior to driving. You should also not need the use of a sling. Studies looking at return to driving after distal radius surgery typically report a timeline from 1-6 weeks, largely dependent on pain control. In general, a patient should possess the strength and range of motion to utilize the vehicles steering wheel in all situations prior to driving.
Post operative Instructions
- Following your stay in the recovery room and when your vital signs are stable you will be discharged to your escort.
- Remember, it is normal to feel a little dizzy or drowsy for several hours after surgery. This is due to the action the medicine used during surgery.
- If you do not have a post operative appointment scheduled, please call the office as soon as possible to schedule this appointment.
- Take your pain medicine as directed. Begin the pain medicine before you start getting uncomfortable, as the nerve block will wear off. If you wait to take your pain medication until the pain is severe, you will have more difficulty in controlling the pain.
- If you are taking narcotic pain medication you may need a stool softener to prevent constipation. Over-the-counter medication such as Docusate or Milk of Magnesia is recommended.
- Notify the office of any fever, chills, or temperature > 100.5.
- Notify the office of any wound drainage.
Post-Surgery Diet
Resume your diet as tolerated and include vegetables, fruits, and proteins (such as meats, fish, chicken, nuts, and eggs) to promote healing. Also, remember to have adequate fluid intake. It is common after surgery to lack an appetite. This may be the result of anesthesia and the medications. Proper nutrition is needed for healing. During the healing process, the body needs increased amounts of calories and protein. Eat a variety of foods to get all the calories, proteins, vitamins, and minerals you need. If you have been told to follow a specific diet, please follow it.
How should I manage my surgical site and bandages?
You will be in a splint after surgery. You should keep this clean and dry until your follow up. Cast covers can be purchased online to aid in keeping the splint dry during showers.
What is my activity level after surgery?
You will use a sling for comfort. It is okay to remove the sling as tolerated and move the elbow. You should not be lifting with the elbow. You are also encouraged to move your fingers as tolerated. Elevation of the hand will aid with swelling.
Can I smoke following surgery?
You should not smoke after surgery as it interferes with healing.
Questions or Concerns
If at anytime you have questions or concerns you can either contact your surgeon’s medical assistant via email or you can call the main office numbers at: 855-624-3306. You can also use the electronic medical record’s online portal to send questions.
Example rehabilitation protocol:
| Post-OP Week 0-2: | Begin: |
|---|---|
| Goals: | 1. Minimize swelling and pain 2. Begin forearm supination and pronation 3. Full elbow and shoulder range of motion |
| Exercises: | 1. AROM Elbow as above 5-6 times per day 2. AROM Shoulder 3. AROM fingers |
| Weeks 2-6: | Begin: |
|---|---|
| Goals: | 1. Improve wrist range of motion to 50% of contralateral side by 6 weeks |
| Exercises: | 1. Week 2: ACTIVE Wrist flexion extension, full hand ROM, active supination/pronation 2. Week 2: begin Putty for grip strength, pulley ROM exercises 3. Week 2: ACTIVE Elbow extension to full, begin supine scapular stabilizations (no weight), door ABCs or Circles with ball 4. Week 2: Initiate submaximal progressive strengthening, such as towel and putty squeezing and light-load gripping exercises 5. Week 2: Clinicians may perform a combination of edema control techniques, including MLD and other manual edema mobilization, exercises, elevation, compression gloves, low-stretch bandaging, and/or iHEP instruction, to induce short-term (2-6 weeks) benefits on hand swelling, AROM, function, and pain following nonoperative and operative DRF management. 6. Week 2: Clinicians should integrate GMI as part of a multimodal management strategy to improve short-term outcomes in pain, AROM, and patient-reported function during the early rehabilitation stage (6-8 weeks) for individuals following nonoperative and operative treatment for DRF. |
| Weeks 7+: | Begin: |
|---|---|
| Goals: | 1. Normalize wrist strength and range of motion |
| Exercises: | 1. Continue strengthening exercises to wrist, forearm, and possibly shoulder, depending on sport and/or work requirements |
References:
- Shen O, Chen CT, Jupiter JB, Chen NC, Liu WC. Functional outcomes and complications after treatment of distal radius fracture in patients sixty years and over: A systematic review and network meta-analysis. Injury. 2023;54(7). doi:10.1016/j.injury.2023.04.054
- van Rossenberg LX, Beeres FJP, van Heijl M, et al. Operative versus non-operative treatment of ulnar styloid process base fractures: a systematic review and meta-analysis. European Journal of Trauma and Emergency Surgery.Springer Science and Business Media Deutschland GmbH. 2024;50(6):2843-2854. doi:10.1007/s00068-024-02660-2
- Suojärvi N, Waris E. Radiographic measurements in distal radius fracture evaluation: a review of current techniques and a recommendation for standardization. Acta radiol.SAGE Publications Inc. 2024;65(9):1065-1079. doi:10.1177/02841851241266369
- Ochen Y, Peek J, Van Der Velde D, et al. Operative vs Nonoperative Treatment of Distal Radius Fractures in Adults: A Systematic Review and Meta-analysis. JAMA Netw Open. 2020;3(4). doi:10.1001/jamanetworkopen.2020.3497
- Suojärvi N, Tampio J, Lindfors N, Waris E. Computer-aided 3D analysis of anatomy and radiographic parameters of the distal radius. Clinical Anatomy. 2021;34(4):574-580. doi:10.1002/ca.23615
- Zhu C, Wang X, Liu M, et al. Non-surgical vs. surgical treatment of distal radius fractures: a meta-analysis of randomized controlled trials. BMC Surg. 2024;24(1). doi:10.1186/s12893-024-02485-1
- Pulos N, Michalik AJ. Common Hand Injuries in the Baseball Player. Curr Rev Musculoskelet Med.Springer. 2023;16(1):19-23. doi:10.1007/s12178-022-09812-0
- Mehta SP, Karagiannopoulos C, Pepin ME, et al. Distal Radius Fracture Rehabilitation. J Orthop Sports Phys Ther. 2024;54(9):CPG1-CPG78. doi:10.2519/jospt.2024.0301
- Schmidt V, Gordon M, Tägil M, Sayed-Noor A, Mukka S, Wadsten M. Association between Radiographic and Clinical Outcomes Following Distal Radial Fractures: A Prospective Cohort Study with 1-Year Follow-up in 366 Patients. Journal of Bone and Joint Surgery. 2023;105(15):1156-1167. doi:10.2106/JBJS.22.01096
- Gutiérrez-Espinoza H, Araya-Quintanilla F, Cuyul-Vásquez I, et al. Effectiveness and Safety of Different Treatment Modalities for Patients Older Than 60 Years with Distal Radius Fracture: A Network Meta-Analysis of Clinical Trials. Int J Environ Res Public Health.MDPI. 2023;20(4). doi:10.3390/ijerph20043697
- Othman S, Shamloul G, Othman A, Pistorio AL. The Impact of Wrist Fractures on Long-Term Basketball Performance. J Hand Microsurg. 2024;16(1). doi:10.1055/s-0042-1757178
- Labrum JT, Ilyas AM. Bridge plate fixation of distal radius fractures: Indications, techniques, and outcomes. Orthopedics.Slack Incorporated. 2021;44(4):E620-E625. doi:10.3928/01477447-20210618-26
- Dario P, Matteo G, Carolina C, et al. Is it really necessary to restore radial anatomic parameters after distal radius fractures? Injury. 2014;45(S6):S21-S26. doi:10.1016/j.injury.2014.10.018
- Wang A, Lefaivre KA, Potter J, et al. Complex regional pain syndrome after distal radius fracture: A survey of current practices. PLoS One. 2024;19(11). doi:10.1371/journal.pone.0314307
- Treatment of Distal Radius Fractures Appropriate Use Criteria.; 2021. https://aaos.webauthor.com/go/auc/terms.cfm?actionxm=Terms&auc_id=225050
- Ando J, Takahashi T, Ae R, et al. Epidemiology of distal radius fracture: a regional population-based study in Japan. BMC Musculoskelet Disord. 2023;24(1). doi:10.1186/s12891-023-06608-2
- Ochen Y, Peek J, Van Der Velde D, et al. Operative vs Nonoperative Treatment of Distal Radius Fractures in Adults: A Systematic Review and Meta-analysis. JAMA Netw Open. 2020;3(4). doi:10.1001/jamanetworkopen.2020.3497
- Dario P, Matteo G, Carolina C, et al. Is it really necessary to restore radial anatomic parameters after distal radius fractures? Injury. 2014;45(S6):S21-S26. doi:10.1016/j.injury.2014.10.018
- Chhabra AB, Yildirim B. Adult Distal Radius Fracture Management. Journal of the American Academy of Orthopaedic Surgeons.Lippincott Williams and Wilkins. 2021;29(22):E1105-E1116. doi:10.5435/JAAOS-D-20-01335
- Haslhofer DJ, Froschauer SM, Gotterbarm T, Schmidt M, Kwasny O, Holzbauer M. Comparison of surgical and conservative therapy in older patients with distal radius fracture: a prospective randomized clinic al trial. Journal of Orthopaedics and Traumatology. 2024;25(1). doi:10.1186/s10195-024-00788-w
- Chung KC, Kim HM, Malay S, Shauver MJ. Comparison of 24-Month Outcomes after Treatment for Distal Radius Fracture. Annu Rev Plant Biol. 2021;4(6). doi:10.1001/jamanetworkopen.2021.12710
- Yang J, Li Y, Li X, Wulan N. A meta-analysis comparing volar locking plates and cast immobilization for distal radius fractures in the elderly. J Orthop Surg Res. 2024;19(1). doi:10.1186/s13018-024-05216-7
- Rosenauer R, Pezzei C, Quadlbauer S, et al. Complications after operatively treated distal radius fractures. Arch Orthop Trauma Surg.Springer. 2020;140(5):665-673. doi:10.1007/s00402-020-03372-z
- Ng CY, Mcqueen MM. What are the radiological predictors of functional outcome following fractures of the distal radius? J Bone Joint Surg [Br]. 2011;93(2):93-145. doi:10.1302/0301-620X.93B2
- Hevonkorpi TP, Launonen AP, Reito A, et al. Nonoperative treatment versus volar locking plating for distal radius fracture in patients aged 65 years or older (DRIFT trial): A randomized controlled trial. PLoS Med. 2025;22(9 September). doi:10.1371/journal.pmed.1004728
- Mizuno K, Sato K, Takahashi G, Mimata Y, Murakami K, Doita M. Three-dimensional imaging of the distal radius with reference to volar locking plate surgery. Orthopaedics and Traumatology: Surgery and Research. 2022;108(7). doi:10.1016/j.otsr.2022.103372
- Ghaddaf AA, Abdulhamid AS, Alomari MS, Alquhaibi MS, Alshehri AA, Alshehri MS. Comparison of immobilization periods following open reduction and internal fixation of distal radius fracture: A systematic review and meta-analysis. Journal of Hand Therapy. 2023;36(1):23-32. doi:10.1016/j.jht.2021.06.004
- Chung SR, Chung KC. Recognizing and Treating Unique Distal Radius Fracture Patterns that are Prone to Displacement. Hand Clin.W.B. Saunders. 2023;39(3):279-293. doi:10.1016/j.hcl.2023.02.004
- Tan CMP, Pillay KDR, Ang ML, Chan ML, Acharyya S, Satkunanantham M. When is it safe to return to driving after distal radius fracture fixation? A prospective study. Journal of Orthopaedic Science. 2024;29(2):537-541. doi:10.1016/j.jos.2023.02.018
- Inclan PM, Dy CJ. How to Treat Distal Radius Fractures: Right Patient, Right Care, Right Time, and Right Cost. Hand Clin.W.B. Saunders. 2021;37(2):205-214. doi:10.1016/j.hcl.2021.02.003
- Doermann A, Gupta DK, Wright DJ, et al. Distal Radius Fracture Management: Surgeon Factors Markedly Influence Decision Making. J Am Acad Orthop Surg Glob Res Rev. 2023;7(3). doi:10.5435/JAAOSGlobal-D-23-00002
- Rabinovich R V., Polatsch DB, Beldner S. Articular Fragment Escape and Carpal Subluxation Following Distal Radius Fracture Fixation. Journal of Hand Surgery.W.B. Saunders. 2024;49(12):1250-1259. doi:10.1016/j.jhsa.2024.07.018
- Larrosa Pardo F, Bondesson E, Petersson IF, Schelin MEC, Jöud A. Prolonged opioid use after distal radius fracture. European Journal of Pain (United Kingdom). 2023;27(7):848-859. doi:10.1002/ejp.2114
- Khan S, Persitz J, Shrouder-Henry J, Khan M, Chan A, Paul R. Effect of Time-To-Surgery on Distal Radius Fracture Outcomes: A Systematic Review. Journal of Hand Surgery. 2023;48(5):435-443. doi:10.1016/j.jhsa.2022.12.018
- Ingall EM, Bernstein DN, Shoji MM, Merchan N, Harper CM, Rozental TD. Using the QuickDASH to Model Clinical Recovery Trajectory After Operative Management of Distal Radius Fracture. J Hand Surg Glob Online. 2021;3(1):1-6. doi:10.1016/j.jhsg.2020.10.001
- Niemann MJ, Lese AB, Sraj S, Taras JS. Distal Ulna Fracture Fixation with the Specialized Threaded Pin. J Hand Surg Glob Online. 2023;5(4):426-429. doi:10.1016/j.jhsg.2023.03.012
- Jones CM, Ramsey RW, Ilyas A, et al. Safe Return to Driving After Volar Plating of Distal Radius Fractures. Journal of Hand Surgery. 2017;42(9):700-704.e2. doi:10.1016/j.jhsa.2017.05.030
- Kärnä L, Launonen AP, Karjalainen T, et al. LIMPER trials: immediate mobilisation versus 2-week cast immobilisation after distal radius fracture treated with volar locking plate - a study protocol for a prospective, randomised, controlled trial. BMJ Open. 2022;12(11). doi:10.1136/bmjopen-2022-064440
- Gottschalk MB, Dawes A, Hurt J, et al. A Prospective Randomized Controlled Trial of Methylprednisolone for Postoperative Pain Management of Surgically Treated Distal Radius Fractures. Journal of Hand Surgery. 2022;47(9):866-873. doi:10.1016/j.jhsa.2022.06.008
- Velmurugesan PS, Nagashree V, Devendra A, Dheenadhayalan J, Rajasekaran S. Should ulnar styloid be fixed following fixation of a distal radius fracture?,. Injury. 2023;54(7). doi:10.1016/j.injury.2023.04.055
- Hess DE, Carstensen SE, Moore S, Dacus AR. Smoking Increases Postoperative Complications After Distal Radius Fracture Fixation: A Review of 417 Patients From a Level 1 Trauma Center. Hand. 2020;15(5):686-691. doi:10.1177/1558944718810882
- Sobel AD, Calfee RP. Distal Radius Fractures in the Athlete. Clin Sports Med.W.B. Saunders. 2020;39(2):299-311. doi:10.1016/j.csm.2019.10.005
- Gutiérrez-Espinoza H, Gutiérrez-Monclus R, Román-Veas J, Valenzuela-Fuenzalida J, Hagert E, Araya-Quintanilla F. Effectiveness of supervised physiotherapy versus a home exercise program in patients with distal radius fracture: a randomized controlled trial with a 2-year follow-up. Physiotherapy (United Kingdom). 2024;124:93-100. doi:10.1016/j.physio.2024.03.005
- de Villeneuve Bargemon JB, Soudé G, Gras M, Lupon, Fruchart E. Physical therapy after distal radius fracture. Hand Surg Rehabil.Elsevier Masson s.r.l. 2023;42(2):168-169. doi:10.1016/j.hansur.2022.12.002
- Warwick D, Smythe L, Fetouh S. Does a distal radial fracture lead to osteoarthritis? Re-examining the evidence for early treatment. Journal of Hand Surgery: European Volume.SAGE Publications Ltd. 2025;50(1):6-14. doi:10.1177/17531934241265839
- Poiset S, Abboudi J, Gallant G, et al. Predictive Factors for Return to Driving following Volar Plate Fixation of Distal Radius Fracture. J Wrist Surg. 2020;09(04):298-303. doi:10.1055/s-0040-1709189
- Larose G, Roffey DM, Broekhuyse HM, Guy P, O’Brien P, Lefaivre KA. Trajectory of Recovery following ORIF for Distal Radius Fractures. J Wrist Surg. 2024;13(03):230-235. doi:10.1055/s-0043-1771045
- Tay K, Bin Abd Razak HR, Yew AKS, Koh JSB, Howe TS. Bony Anatomy around the Watershed Line of the Distal Radius. J Wrist Surg. 2021;10(04):276-279. doi:10.1055/s-0040-1719031
- Mulakaluri A, Julian KR, Fernandez A, Kamal RN, Shapiro LM. Are Clinical Practice Guidelines Representative of Patients With Distal Radius Fractures? A Review of Patient Demographics and Patient-Reported Outcome Measures Used to Inform Guidelines. Journal of Hand Surgery. 2024;49(7):649-655. doi:10.1016/j.jhsa.2024.03.015
- Farrell N, Greenfield PT, Rutkowski PT, Weller WJ. Perioperative Pain Management for Distal Radius Fractures. Orthopedic Clinics of North America.W.B. Saunders. 2023;54(4):463-470. doi:10.1016/j.ocl.2023.05.006
- Niedermeier SR, Crouser N, Hidden K, Jain SA. Pain Management following Open Reduction and Internal Fixation of Distal Radius Fractures. J Wrist Surg. 2021;10(01):027-030. doi:10.1055/s-0040-1716508




